Case reports of patients helped by therapy,
Say you see 100 adult patients this week. How many have a sexual dysfunction? 10? 20? Would you believe 43? In a National Health and Social Life Survey1 of 1,749 women and 1,410 men aged 18 to 59 years, 43% of women and 31% of men reported sexual dysfunction. Rates that high make sexual dysfunction an important public health concern—one that is highly associated with impaired well-being and negative experiences in sexual relationships.
Similar findings marked a study2 of general practice patients in Britain: 41% of 979 women and 34% of 789 men reported sexual dysfunction. Although 52% wanted professional help, only 10% had received it.
As primary care providers, Ob/Gyns must identify common problems, treat those within our expertise, and refer the others. In all likelihood, we are the first physicians women see about a sexual problem. For these reasons—and because dysfunction is so common—it is appropriate that we screen for and address female sexual dysfunction.
This article presents a medical model of management and tells how to take a sexual history, formulate a differential diagnosis, manage common sexual problems, and identify indications for referral.
The medical model
According to the medical model, a patient presents with a problem, which is investigated by history and physical examination. A differential diagnosis is formulated, and appropriate laboratory tests or other evaluations are conducted. The patient’s problem is compared to a normal physiologic process to determine pathophysiology. Diagnosis and therapy follow.
The medical model for sexual dysfunction is the same as that for any disease, such as asthma, in which normal breathing is interrupted. In the sexual response cycle, physiologic changes can be measured and specifically described, as Masters and Johnson explained in 1966 in Human Sexual Response (FIGURE 1). Any barriers that interrupt this progression “block” the normal response cycle, resulting in sexual dysfunction. We aim to identify and remove or get around any barriers.
FIGURE 1 Use the sexual response cycle in dialogue with the patient
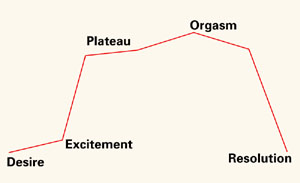
Most patients with sexual dysfunction can identify the phase in the Masters and Johnson sexual response cycle where normal progression is interrupted. Using a sketch of this cycle helps patients understand and articulate their problem.
The sexual response cycle
Desire initiates the cycle, followed by the excitement phase, during which breathing rate and pulse increase, blood flow shifts away from muscles and into the skin and pelvic organs, and there is an associated expansion, lengthening, and lubrication of the vagina. A plateau follows, during which there is no further increase in signs such as increased pulse rate. Orgasm is the first point in the response cycle that is different in men and women. Men have an obligatory resolution phase and return to baseline state; women can return to the plateau state and then have another orgasm. The resolution phase lengthens in duration in both sexes with increasing age.
The sexual response cycle is innate, like any physiologic process. It cannot be taught or learned, and is not under voluntary control. It is critical that patients understand that the sexual response cycle is a natural function that everyone has—just as everyone has innate capacity to breathe. Patients do not learn it, any more than they have to learn respiration.
Sexual behavior, however, is learned, and sexual dysfunctions are exhibited by behavior. Sex therapy is a learning process, the aim of which is to change the behavior. Sexual dysfunctions have both cognitive and physical components; although response is physiologic, it can be altered by emotion, as can respiration.
The relationship is the patient. Sexual dysfunction occurs within a relationship, and the relationship needs and stands to benefit from therapy.
Reassuring anxious, angry patients
Approach is critical, and must reflect an understanding that sexual dysfunction is real. Many patients have been told that the problem is “all in their head” or that they are deliberately acting dysfunctionally.
Confrontation and support are useful communication tools. Confrontation means identifying behaviors and beliefs and how beliefs influence behaviors. Support means conveying to the patient that you understand that she is in distress and that it couldn’t have happened any other way for her.
A “therapeutic mirror” technique can show the patient her beliefs, attitudes, and behaviors. The therapist repeats the the patient’s beliefs and behaviors until the patient states that they are an accurate reflection, or tells the therapist what is inaccurate.
Assure the patient that anxiety is to be expected, and that her probelm is common and treatable. These patients believe they have thought of everything, and nothing has worked. Just reassuring them may help.