Although UAE is generally not performed in women who wish to preserve their fertility, it is sometimes used in fibroid patients when myomectomy is contraindicated because of the size and/or number of fibroids.11,22,23 Only a few small series and case reports describe successful pregnancies following UAE.
For example, in a study involving 400 women, McLucas et al22 reported 17 pregnancies in 14 women among 149 patients who stated a desire for fertility after UAE. Of these, 5 spontaneous abortions were observed, and 10 women had normal term deliveries. No perfusion or other problems were reported during pregnancy or labor.
Goldberg and colleagues23 analyzed 50 published cases of post-UAE pregnancies and found higher rates of cesarean delivery, preterm birth, malpresentation, small-for-gestational-age infants, spontaneous abortion, and postpartum hemorrhage than in the general population, though the reasons were unclear.
In our experience at the New England Fibroid Center, 5 of 12 patients below the age of 40 who wanted to preserve fertility became pregnant and successfully delivered full-term infants.
In general, the risks of infertility, premature ovarian failure/menopause, radiation exposure, and hysterectomy following UAE are small and compare favorably with those associated with myomectomy. Fertility rates are similar to those for women undergoing myomectomy.24
Nevertheless, well-controlled studies and additional data are needed before UAE can be confidently recommended as a first-line approach for preserving fertility.11
Treating adenomyosis
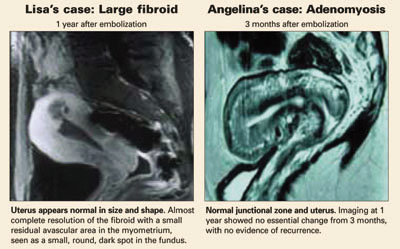
ANGELINA’S CASE
Adenomyosis resolves
During Angelina’s UAE procedure, angiographies showed enlarged right and left uterine arteries with numerous prominent intrauterine branches supplying the enlarged uterus. After UAE with PVA microspheres, post-embolization angiograms showed occlusion of the right and left uterine arteries and their branches.
Her symptoms resolved completely following the procedure. One year later, a follow-up MRI showed normal uterine size and shape, with complete resolution of adenomyosis.
Several small series have reported successful treatment of women with symptomatic adenomyosis. For example, of 23 women who underwent UAE for this indication, Chen and colleagues9 reported:
- Complete resolution of dysmenorrhea in 19 women and significant improvement in 2. Two other patients had recurrent symptoms.
- A substantial decrease in uterine volume in most of the women.
- An immediate decrease in intrauterine blood flow detected by color Doppler ultrasonography.
In a prospective study10 involving 18 women with symptomatic adenomyosis:
- 94% had diminished menorrhagia 6 months after UAE, and 94% had a slight decrease (mean: 15%) in uterine volume.
- After 1 year, 73% of women had diminished menorrhagia, and 53% had complete resolution.
- After 2 years, 56% of women had complete resolution of menorrhagia, 44% required additional treatment due to failure or recurrence, and 28% underwent hysterectomy.
In our limited experience with adenomyosis at the New England Fibroid Center, we saw no significant difference in technical success rates (100%) after UAE, compared with fibroid patients. However, there was a relatively high recurrence rate (2 of 6 patients) of presenting symptoms (menorrhagia or dysmenorrhea), and 2 patients later underwent hysterectomy.
Well-controlled studies are needed before UAE can confidently be recommended for symptomatic adenomyosis.
The authors report no financial relationships relevant to this article.