Once the peritoneum is entered, bluntly extend the incision laterally to the uterosacral ligaments, and place a weighted Steiner-Auvard retractor in the incision.
Dissect first, then divide the ligaments
When leiomyomata are present, anatomical distortion tends to be limited to the fundus; cervical anatomy remains relatively unaltered. After completing the circular cervical incision, dissect the vesicocervical and vesicouterine spaces. Some sharp dissection is usually required at the level of the pericervical ring—the supravaginal septum—which consists of dense fibroelastic connective tissue. Place a Heaney or Breisky-Navratil retractor within the anterior incision to obtain full cervical access.
Next, sequentially clamp, divide, and ligate the uterosacral, cardinal, and pubourethral ligaments. Once this task is done, the vascular bundle containing the uterine artery and veins becomes accessible; divide it as well.
If the anterior peritoneum has not been passively entered, it can now be easily incised.
Now that the suspensory apparatus and the major blood supply have been divided, uteroreductive techniques can be employed.
No absolute size limit
There is no objective limit to the size of a uterus that can be safely removed using reductive techniques. Generally, extra skill and experience are needed to remove an organ larger than 12 weeks’ size (approximately 280 g). Numerous reports document the safe removal of enlarged uteri, even those larger than 1,000 g.5-17
Uterine size is reduced in 3 ways: morcellation, coring, and/or cervicectomy.
The best method varies from case to case, depending on the specific uterine anatomy and the surgeon’s skill. Often, more than 1 debulking technique is used in a single case.
Do not begin debulking until peritoneal access is attained, the paracolpium is divided, and the uterine artery is ligated.
Morcellation is well suited to multiple fibroids
First, sharply divide the cervix, cutting vertically in the midline, and extend the incision into the uterine fundus using the endocervical canal and endometrial cavity as visual guides for the incision (FIGURE 2A). As leiomyomata are encountered, grasp each with a Myotome grasper (Marina Medical, Hollywood, Fla) and remove them with Myotomes (Marina Medical). Both the spoon-tipped and chisel-tipped Myotomes have dissecting tips that allow rapid and precise enucleation of tumors. The tip is sharp enough to dissect the capsule of the myomata, but not so sharp that it endangers adjacent structures.
Continue to remove the fibroids as they become accessible. If incisions into the serosa of the uterus are necessary to remove palpable subserosal tumors, make the incisions under direct vision. Access to the serosa usually is greater on the posterior surface of the uterus. With adequate retraction, the anterior surface can also be incised.
If a bulky uterus prevents immediate access to leiomyomata, one strategy is to remove elliptical wedges of myometrium adjacent to the uterine bisecting incision. The Martin myomectomy scissors (Marina Medical) have serrated edges originally designed by orthopedists to cut cartilage, as well as sharp tips that can be inserted into a tumor prior to cutting. They help debulk large myomata (FIGURE 2B) and can be used to quickly remove wedges of myometrium. After sufficient debulking, large myomata can be removed safely (FIGURE 2C).
This morcellation method minimizes the need to use a knife in the “invisible” upper reaches of the fundus. Continuous downward traction on the divided cervix prevents bleeding, and the gradual reduction in size of the debulked fundus allows for sufficient descent of the uterus; it also permits posterior rotation. Ultimately, it becomes possible to clamp the utero-ovarian pedicles and to completely remove the uterus.
In most cases, the uterine serosa can be left intact using morcellation. The size of the uterus that can be removed using this technique is limited only by the experience of the surgeon (FIGURE 3).
FIGURE 2 Expose, debulk, and remove the dominant myoma
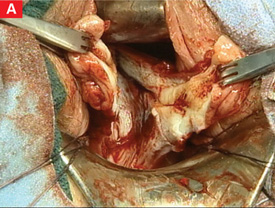
Incise the cervix along the midline to gain access to the fundus and expose the dominant myoma.
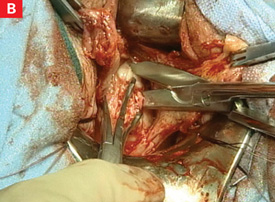
Insert the sharp tip of the scissors into the myoma prior to cutting.
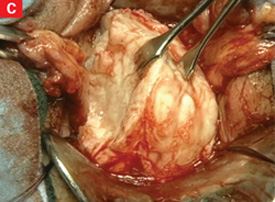
When the myoma has been sufficiently debulked, remove it through the vagina.
FIGURE 3 Massive uteri can be removed vaginally

This uterus and multiple myomata were removed from a single patient using the vaginal route.
Use coring for moderately enlarged uteri
This is a useful technique when the uterus contains multiple small leiomyomata, a single dominant tumor, or cicatrized adenomyosis. Begin by making a circular incision into the fundus of the uterus just above the isthmus. The incision should be parallel to the central axis of the endometrial cavity.18
Apply firm downward traction on the cervix to allow the portion of the uterus central to the incision to evert. Continue to incise the uterus in a circular pattern to allow more of the bulk of the fundus to descend.