Port placement in the patient who has a large uterus is the same as it is for other laparoscopic hysterectomies in our practice. We use an 11-mm trocar at the umbilicus for a 10-mm endoscope. We use the 10-mm endoscope because the light it provides to the surgical field is superior to that of a 5-mm endoscope, and the 10-mm scope is more durable.
We place a 5-mm trocar just above the anterior iliac crest on each side, lateral to the ascending inferior epigastric vessels (FIGURE 2). We place an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port on the side of the primary surgeon. This trocar serves a dual purpose: It is the primary port for the surgeon, and removal of the trocar sleeve later in the procedure allows for easy insertion of the morcellator.
Some patients will require a fifth port on the side opposite the primary surgeon to allow better access to the uterine blood supply or to facilitate uterine manipulation.
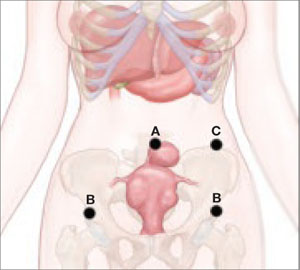
FIGURE 2 Port placement when the uterus is large
A midline umbilical port (A) is possible even when the uterus is large. Other ports include a 5-mm trocar just above the anterior iliac crest on each side (B), and an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port nearest the primary surgeon (C).
Why an angled scope is superior
Many gynecologists fear laparoscopic surgery in patients who have a large uterus. The reason? Poor visualization of the surgical field. However, the type of endoscope that is used has a bearing on visualization.
Most gynecologists are trained to use a 0° endoscope for laparoscopic surgery. However, when the uterus is large, the 0° scope yields an inadequate field of view, whether the endoscope is placed at the umbilicus or through a lateral port. Critical structures like the vascular bundles, ureters, and even the bladder may be inadequately visualized using the 0° endoscope (FIGURE 3).
Gynecologists routinely use angled scopes in hysteroscopy and cystoscopy, but tend to avoid them in laparoscopy because of difficulty orienting the surgical field. As gynecologists, we readily accept that use of an angled scope in hysteroscopy and cystoscopy requires rotation of the scope while the camera maintains its horizontal position. The same concept applies to laparoscopy.
Use of the angled scope in the abdomen is a two-step process. First, it must be rotated to achieve the desired field of view. Then, as the endoscope is held firmly to maintain this view, the camera head must be rotated on the scope to return the field to a horizontal position.
Many surgeons find this action difficult because they or the assistant are holding the camera in one hand and an instrument in the other. We solve this problem by using a mechanical scope holder to secure the camera and endoscope in the position we desire.
In some cases, the camera head does not attach securely to the eyepiece, and the scope rotates on the camera as soon as it is released. This difficulty arises when the eyepiece of the endoscope is slightly smaller than the camera attachment. The problem is easily solved by placing a small piece of surgical skin closure tape on one edge of the eyepiece, slightly increasing its diameter. The camera attachment then holds the scope securely.
Human scope holders may tire during long cases, causing field drift at critical moments. In contrast, a mechanical scope holder is easily and intermittently adjusted for field of view, producing a steady field of view and minimizing the impact of manual manipulation of the scope on surgical outcome. It also allows the surgeon and first assistant to use two hands while operating.
General surgeons and urologists often use 30° endoscopes. Gynecologists working in the pelvis see better using a 45° scope (FIGURE 3). Most ORs offer a 30° endoscope but do not always have a 45° endoscope available in the instrument room. This is regrettable. Compared with the 30° scope, the 45° instrument provides better visual access to the low lateral uterine blood supply and bladder flap, particularly when the patient has a globular uterus or large, low anterior fibroid. We include both 5-mm and 10-mm 45° endoscopes in our laparoscopic tool chest, and believe they are essential options.
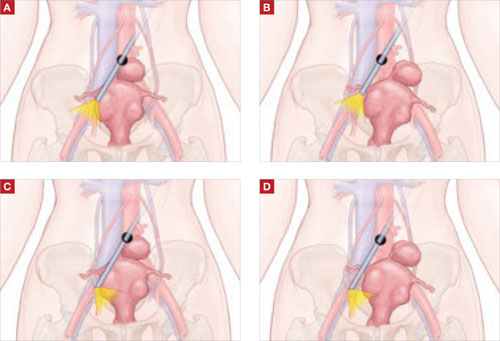
FIGURE 3 The 45° laparoscope provides better visual access
(A) 0° scope, uterus midline: Right broad ligament view obstructed. (B) 0° scope, uterus to left: Right broad ligament view still obstructed. (C) 45° scope, uterus midline: Right broad ligament view improved. (D) 45° scope, uterus to left: Right broad ligament view optimal.