The authors report no financial relationships relevant to this article.
Barbed suture is a relatively new technology that has the potential to greatly facilitate laparoscopic suturing. Two barbed sutures, each a different type, are available, or soon will be:
- the Quill bidirectional barbed suture (Angiotech Pharmaceuticals) was approved by the US Food and Drug Administration (FDA) in 2004 for soft-tissue approximation and has been sold in the United States since 2007 ( FIGURE 1A )1
- the V-Loc 180 unidirectional barbed suture (Covidien) won FDA approval in March for soft-tissue approximation. It should be available in October ( FIGURE 1B ).
(Note: We have performed laparoscopic surgery using the Quill suture, but not the V-Loc 180, both as part of clinical research and in practice.)
In the bidirectional suture, barbs are cut into suture in a direction opposite to the needle; the barbs change direction at the midpoint of the suture, and needles are swaged onto both ends ( FIGURE 1A ).2
The anchoring of bidirectional barbed suture resists migration and can be conceptualized as a “continuous interrupted” suture without knots; it has been shown to have tissue-holding performance that is at least equal to knot-anchored suture.3,4
A suture with bidirectional barbs offers several advantages:
- Because it self-anchors and is balanced by the countervailing barbs, no knots are required
- It self-anchors every 1 mm of tissue, yielding more consistent wound opposition; this may result in a more “watertight” seal
- Because it is knotless, it can securely reapproximate tissues in less time, at less cost, and with less aggravation.5,6
Note: Whether these characteristics apply to unidirectional barbed suture remains to be determined.
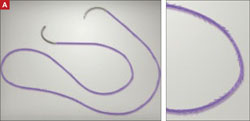
FIGURE 1 Two types of barbed suture
Bidirectional suture, in which barbs are cut into suture and change direction at the midpoint.

Unidirectional suture has a loop at the distal end to facilitate initial suture fastening.
Specifications
Because the effective diameter of suture is decreased when barbs are cut into it, barbed suture is rated one suture size smaller than smooth suture. A 0 barbed suture, for example, equals a 2-0 smooth suture.
In the current version of the Quill suture, there is a segment of approximately 7 cm of smooth suture proximal to each needle. A second-generation Quill will be released this year, with barbs extending all the way to the needles. Bidirectional barbed suture materials currently include polydioxanone (PDO), poliglecaprone 25 (Monoderm), nylon, and polypropylene.
The V-Loc 180 is a unidirectional barbed polyglyconate (Maxon) suture with a loop at the distal end to facilitate initial fastening.
We have performed more than 200 laparoscopic surgeries using Quill suture since March 2008; most involved total laparoscopic hysterectomy and laparoscopic myomectomy. We have also used Quill suture for laparoscopic sacrocolpopexy and uterosacral ligament suspension.
We have had outstanding clinical results: no cuff evisceration and only minor cases of vaginal bleeding or spotting in the immediate postoperative period.7 In one case, reoperation was necessary after laparoscopic myomectomy, but the repeat surgery was performed to treat small-bowel obstruction that was not directly related to the hysterotomy repair.
Technique
For vaginal-cuff closure, we use 0 PDO suture on a 36-mm half-circle taper-point needle. We initially used half of a 14×14-cm suture with a LapraTy clip on the distal end. We began the repair at the distal end of the vaginal cuff, taking care to incorporate the uterosacral ligament into the initial bite, and continuing proximally until the other uterosacral ligament was incorporated into the repair.
More recently, we have been using the 7×7-cm 0 PDO because it is now available with the 36-mm half-circle taper-point needle. Regardless of suture material, it is important to obtain a full-thickness bite, with a 1-cm margin on the vaginal mucosa on each bite.
With the shorter suture, we begin closure in the middle of the cuff and take each needle to the opposite end of the cuff ( FIGURE 2 ). We incorporate the uterosacral ligament into the final bite on each side, and we cut the suture without a knot or a LapraTy clip.
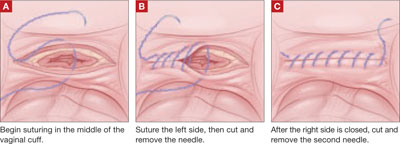
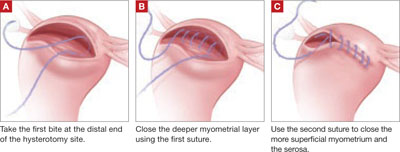
FIGURE 2 Closing the vaginal cuff with bidirectional barbed suture For myomectomy closure, we use 14×14-cm 0 PDO suture on a 36-mm half-circle taper-point needle. If the hysterotomy is longer than 8 cm, we prefer to use 24×24-cm suture. We tack the first needle to the opposite anterior abdominal wall to avoid having the suture become entangled. We close the deepest layer using the first needle; we use the second needle to close the more superficial layer and the serosa, if possible ( FIGURE 3 ). If the suture is used beyond the barbed portion, we cut the needles and apply a LapraTy clip. Sometimes, three or four layers are needed to close a deep myometrial defect. 2/0 Monoderm can also be used for the serosa, continuously or as a baseball stitch.