I enjoyed the recent editorial by Dr. Barbieri and Dr. Clark on the relationship between ovarian teratoma and encephalitis. Little did I know it would come in handy right away.
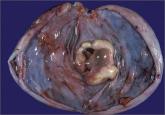
Recently, we were asked to see and operate on a 27-year-old patient with sudden onset of hallucinations, personality changes, and eventually a catatonic-like state (developed over 3 weeks but didn’t require intubation). All testing was negative for viral/bacterial encephalitis. A positive anti-N-methyl-D-aspartate (anti-NMDA)-receptor antibody screen and pelvic imaging revealed a probable teratoma in the right ovary.
We removed the right ovary. The teratoma was small but did have mature neural elements. The patient received the medical treatment outlined by Drs. Barbieri and Clark in their editorial. At the time of this writing, the patient is 3 weeks postsurgery and is talking, walking, eating, and will complete her rehab stay in the next week or so. Truly a remarkable improvement with notable progress every day.
Amazing such a case would arise shortly after I read this editorial—thank you!
John B. Gebhart, MD, MS
Mayo Clinic, Rochester, Minnesota
Dr. Clark and I thank Dr. Gebhart for alerting readers to his recent, very interesting, case of anti-NMDA-receptor antibody-induced encephalitis occurring in a woman with an ovarian teratoma. We hope that she recovers and can return to her full activities as quickly as possible.
I thank Dr. Andrew M. Kaunitz for stating in his January 2014 commentary on estrogen therapy:
For menopausal women who elect to use an oral estrogen, estradiol appears to be a wise choice for both safety and economy. A 1-month supply of 1-mg estradiol tablests costs $4 at some chain pharmacies, whereas 0.625-mg tablets of conjugated equine estrogens cost $84.92.
Human ovaries produce estradiol. Therefore, when production wanes, it makes sense to supplement (not replace!) with estradiol. That’s why I have been prescribing estradiol for many years rather than the more fashionable, trendy conjugated equine estrogens (Premarin, Pfizer).
This situation is similar to thyroid hormones. Again, we use supplementation in case of deficiency; replacement for surgical removal. Semantics is important.
Yasuo Ishida, MD
St. Louis, Missouri
I appreciate Dr. Ishida’s thoughtful comments. It seems that in our practices, we are in agreement regarding our preferred oral estrogen.
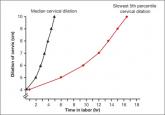
I don’t agree with Dr. Barbieri’s December editorial on the progress of labor. There is pushing, and then again there is pushing. All I seem to experience for my patients after 3 hours is marked perineal edema, not to mention the challenge of an impacted head when ultimately one does proceed with cesarean delivery. Persisting for more than 5 hours is not for me—or my patients.
Eugene Scioscia Jr., MD
Pittsburgh, Pennsylvania
I agree with Dr. Scioscia: Extending the hours of pushing is often accompanied by increasing edema and tissue friability in the birth canal and perineum.
The length of the second stage is not synonymous with “hours of pushing” and the data presented in the editorial focused on the length of the second stage.
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com Please include your name, city and state.