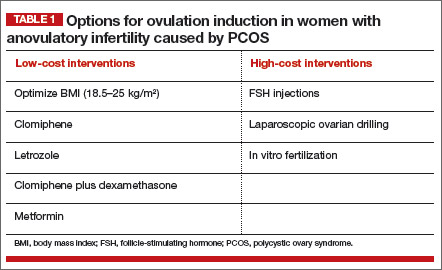
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
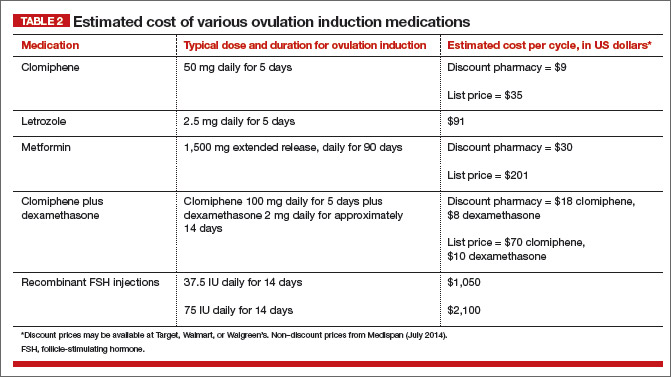
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.