Patients with psoriatic arthritis taking methotrexate demonstrated an improvement in peripheral joint disease, skin disease, enthesitis, dactylitis, and nail disease over 12 weeks in a subanalysis of methotrexate users in the TICOPA (Tight Control of Psoriatic Arthritis) study.
Out of the original 206 patients in the open-label, randomized, controlled TICOPA study, the subanalysis involved 188 who received methotrexate in its first 12 weeks. Substudy authors Dr. Laura C. Coates and Dr. Philip S. Helliwell of the Leeds Institute of Rheumatic and Musculoskeletal Medicine at the University of Leeds (England) verified a maximum dose at 12 weeks of at least 15 mg/week in 175, 20 mg/week in 122, and 25 mg/week in 86 (J Rheumatol. Dec 15. doi: 10.3899/jrheum.150614).
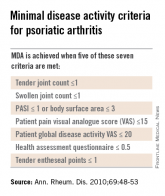
The proportions of patients achieving American College of Rheumatology (ACR) outcomes at 12 weeks were 40.8% for ACR20, 18.8% for ACR50, and 8.6% for ACR70. A total of 22.4% achieved minimal disease activity, defined as meeting five of these seven criteria: 0-1 tender joints, 0-1 swollen joints, Psoriasis Area and Severity Index (PASI) of 1 or less or body surface area involvement of 3 or less, patient pain visual analog score (VAS) of 15 or less, patient global disease activity VAS of 20 or less, health assessment questionnaire of 0.5 or less, and 0-1 tender entheseal points.
Other improvements that occurred at 12 weeks included 27.2% reaching a PASI75, a 62.7% drop in dactylitis incidence, a significant drop of –59.7 in Leeds dactylitis instrument median score, and a significant decrease in the proportion of patients with enthesitis (25.7%). However, the median change in enthesitis score was 0.
Response rates did not differ between patients receiving methotrexate 15 mg/week or higher doses, although there was generally a higher proportion who met various response criteria among those taking greater than 15 mg/week. However, the authors noted that there could be an underestimation of the dose effect because the design of the TICOPA study, which randomized patients to a protocol for tight control of psoriatic arthritis disease activity or standard care, introduced a bias by intentionally escalating treatment doses in patients who continue to have active disease.
The investigators advised that the study results be interpreted in the context of the open-label design of the study, and placed alongside the other observational studies that support its use in psoriatic arthritis.
No relevant conflicts of interest were disclosed.