Massive ventral hernias should be defined as those with a length or width of at least 15 cm and/or an overall area of 150 cm2, according to a report published in the Journal of American Surgery.
Until now, there has been no standardized definition of these defects. Defining massive ventral hernias is the first step in collecting and analyzing data on outcomes so that the best-practice methods for managing these cases can be determined, said Dr. Samuel W. Ross and his associates in the division of gastrointestinal and minimally invasive surgery, Carolinas Medical Center, Charlotte, N.C.
Their results suggest that patients with a massive ventral hernias “can be expected to stay in hospital for approximately 8 days, have an approximately 25% wound complication rate, have an 80% rate of activity limitation, and have a 100% rate of symptomatic pain at 1 month after surgery. This not only requires a long hospital course, with incumbent morbidity, but also the subsequent follow-up and management of wound and other complications,” the investigators said.
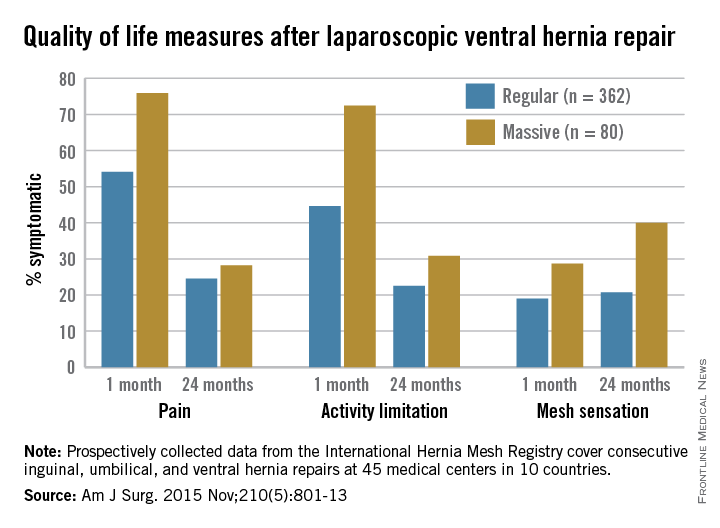
As expected, patients with massive ventral hernias had more complications and lower postop quality of life in terms of pain, activity limitation, and “mesh sensation,” compared with patients having regular hernia.
Large hernia defects are defined in the literature as up to 10 cm in size, but Dr. Ross and his colleagues hypothesized that massive hernia needed a more accurate cutoff size. The goal of this study was to define massive ventral hernia as 15 cm or more intraoperative defect size in any dimension or area 150 cm2 or more, and validate it by comparing ventral hernia repair patients’ outcomes using an international, multicenter, prospectively collected database.
To validate that their definition correlated with patient outcomes, the investigators analyzed information in the International Hernia Mesh Registry, a prospectively collected database covering consecutive inguinal, umbilical, and ventral hernia repairs at 45 medical centers in 10 countries. They focused on 878 cases of ventral hernia treated during a 6-year period. A total of 158 cases (18%) met their criteria for massive ventral hernia.
Hernia repairs were nearly equally divided between laparoscopic (50.3%) and open (49.7%) surgeries. Approximately 18% of each group were massive ventral hernias.
Overall, there were 118 wound complications, including seromas (affecting 9.6% of patients), hematomas (2%), and superficial and deep surgical site infections (2%). Other complications included deep vein thrombosis (0.5%), pneumonia (1%), cardiac events (0.5%), and problems requiring reoperation (4.2%). At 2-year follow-up, 1.5% of the study participants had died and 5.1% had ventral hernia recurrences.
As expected, compared with patients who had regular-sized hernias, those with massive hernias were significantly more obese, had a higher percentage of previous hernia surgeries, and had larger defect sizes. In general, their outcomes were not as good as those of patients with regular-sized hernias.
In the laparoscopic group, patients with massive hernias required a longer length of hospital stay than did those with regular-sized hernias (4.8 vs. 2.6 days), but their rates of wound complications, deep vein thrombosis, cardiac events, reoperation, and recurrence were similar. They had significantly increased pain and limitation of activity for the first postoperative month, but thereafter these factors were comparable.
In the open-surgery group, patients with massive hernias required a longer length of stay and had significantly more hematomas, deep infections at the surgical site, other wound complications, and cases of pneumonia. But their rates of superficial surgical site infection, seroma, cardiac events, hernia recurrence, and death were comparable with those in patients with regular-size hernias. They had significantly increased pain and limitation of activity during the first postoperative month, but thereafter, these factors were comparable (Amer J Surg. 2015;210[5]:801-13).
Interestingly, massive hernias were associated with “increased mesh sensation” at both 1-year and 2-year follow-up only in the laparoscopic cohort. “This finding may be due to the lack of closure of the musculofascial abdominal wall during these laparoscopic repairs, which may allow the patients to directly appreciate the mesh underneath their subcutaneous tissue.” In contrast, open surgery allowed more complete closure of the abdominal wall, “which may have impacted the patients’ perception of the mesh in their abdomens,” Dr. Ross and his associates wrote.
The study had no outside funding. Dr. Ross reported having no relevant financial disclosures. His associates reported ties to W.L. Gore, Ethicon, Novadaq, Bard/Davol, and LifeCell; one associate reported holding a patent for a free mobile app predicting the rate and cost of wound complications after ventral hernia repair, for which he receives no financial gain.