Authors’ Disclosure Statement: The authors report no actual or potential conflict of interest in relation to this article.
Dr. Alvi is an Adult Joint Reconstruction Orthopedic Surgeon, Barrington Orthopedic Specialists, Schaumburg, Illinois. Dr. Thompson is Assistant Professor, Department of Orthopaedic Surgery, and Associate Director, Center for Cerebral Palsy, David Geffen School of Medicine, The University of California, Los Angeles, Los Angeles, California. Dr. Krishnan is a General Surgery Resident, Lenox Hill Hospital/Northwell Health, New York, New York. Dr. Kwasny is Professor of Preventive Medicine, Department of Preventive Medicine, Biostatistics Collaboration Center, Northwestern University, Chicago, Illinois. Dr. Beal is Associate Professor and Program Director; and Dr. Manning is Associate Professor and Vice Chairman Department of Orthopaedic Surgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Address correspondence to: Hasham M. Alvi, MD, Barrington Orthopedic Specialists, 929 W. Higgins Road, Schaumburg, IL 60195 (tel, 847-285-4200; email, Halvi@barrringtonortho.com).
Hasham M. Alvi, MD Rachel M. Thompson, MD Varun Krishnan, MDMary J. Kwasny, ScD Matthew D. Beal, MD David W. Manning, MD . Time-to-Surgery for Definitive Fixation of Hip Fractures: A Look at Outcomes Based Upon Delay. Am J Orthop.
September 7, 2018
References
RESULTS
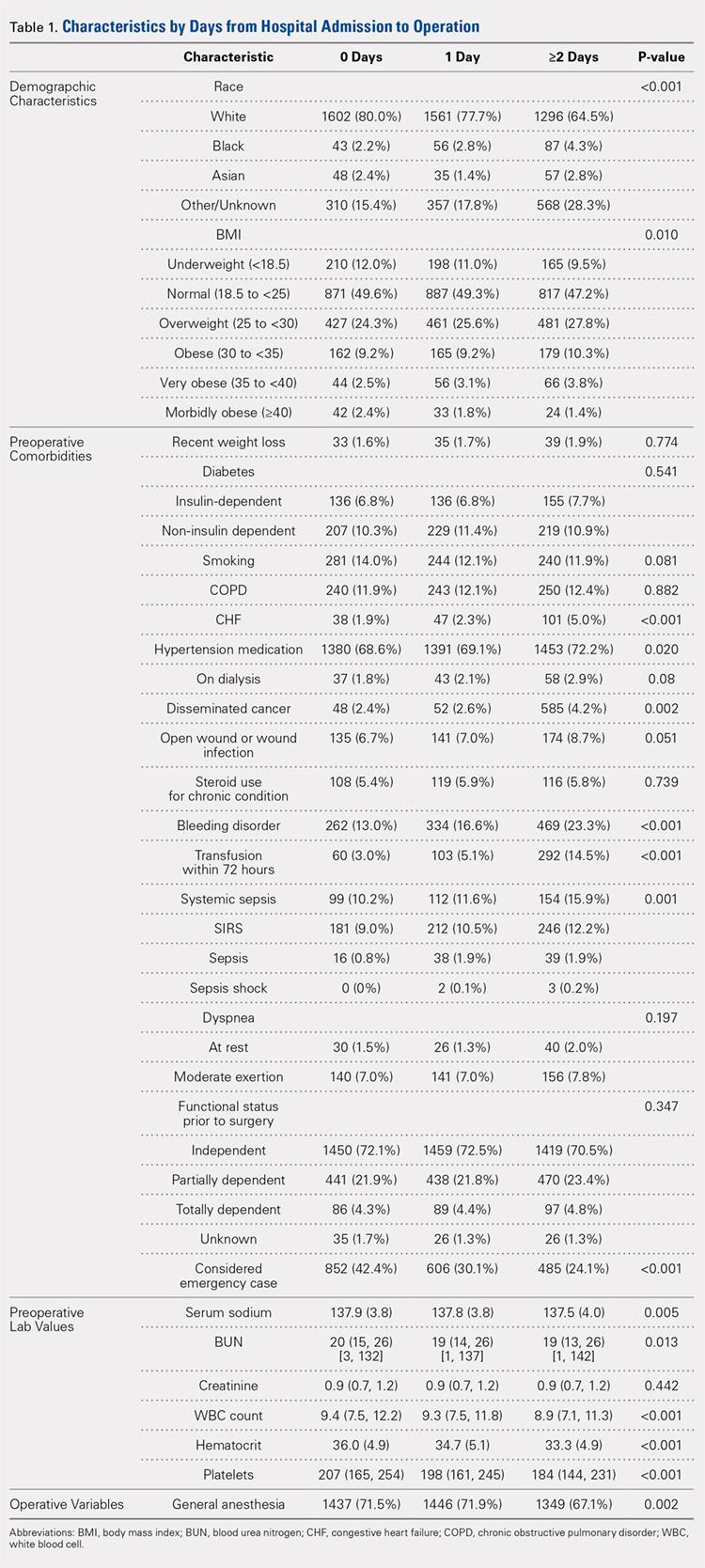
A study population of 6036 hip fractures was identified and divided into 3 groups of 2012 subjects each based upon time-to-surgery. The groups were successfully matched for surgery type, age (≥75 years old), gender, and ASA class. In each group, 594 of the 2012 (29.5%) patients were male, 1525 (75.8%) were ≥75 years of age, 9 (.5%) were ASA Class I, 269 (13.4%) were ASA Class II, 1424 (70.8%) were ASA class III, and 309 (15.4%) were ASA class IV.
Significant differences in preoperative comorbidity burden and preoperative lab values were identified between the 3 cohorts. Increased time-to-surgery was associated with differences in race (P < .001), elevated BMI (P = .010), higher rates of congestive heart failure (P < .001), hypertension medication (P = .020), bleeding disorders (P < .001), blood transfusion within 72 hours of surgery (P < .001), and systemic sepsis (P = .001). Delay to surgery was also associated with lower preoperative sodium (P = .005), blood urea nitrogen (P = .013), serum WBC (P < .001), hematocrit (P < .001), and platelets (P < .001) (Table 1).
The unadjusted analyses revealed no association between time-to-surgery and return to OR (P = .554) nor readmission (P = .285). However, increasing time-to-surgery was associated with an increase in overall complications (P = .034), total length of hospital stay (P < .001), and 30-day mortality (P = .039) (Table 2).
Table 2. Estimated Event Rates from Matched Cohorts (Unadjusted)
Time From Presentation to Definitive Fixation
Outcomes
<24 hours
24-48 hours
>48 hours
P-value
Overall complication rate
15.30%
15.30%
17.90%
0.034
Total length of stay
5.4
6.7
10.9
<0.001
(mean days, 95% confidence interval)
(5.2, 5.7)
(6.5, 7.0)
(10.3, 11.5)
Time from OR to discharge
-ref-
0.96
0.74
<0.001
(Hazard ratio)
(0.90,1.02)
(0.69, 0.79)
Return to OR
2.40%
2.40%
2.00%
0.554
Readmission
9.60%
8.40%
8.30%
0.285
30-day mortality rate
5.80%
5.30%
7.20%
0.039
Abbreviation: OR, operating room.
The adjusted analysis controlling for preoperative demographic and comorbidity variables revealed trends toward the increased overall complications and 30-day mortality with increased time-to-surgery; these trends showed no statistical significance (P = .143 and P = .08). No statistical relationship was observed between return to OR nor readmission and time-to-surgery. Increasing time-to-surgery remained significantly associated with the increased total length of hospital stay (P < .001). The adjusted analysis also revealed that the delay of >48 hours in time-to-surgery resulted in a longer surgery-to-discharge time (P < .001) (Table 3). No evidence of violation of the proportional hazards assumption was observed in the unadjusted nor adjusted clustered proportional hazards models (Wald test, P = .27 and P = .25, respectively).
Table 3. Estimated Event Rates from Matched Cohorts (Adjusteda)
Time from Presentation to Definitive Fixation
Outcomes
<24 hours
24-48 hours
>48 hours
P-value
Overall complication rate
11.70%
10.70%
12.60%
0.143
Total length of stay
4.2
5.1
7.6
<0.001
(mean days, 95% confidence interval)
(4.0, 4.5)
(4.8, 5.5)
(7.1, 8.3)
Time from OR to discharge
-ref-
1.03
0.87
<0.001
(Hazard ratio)
(0.97, 1.09)
(0.81, 0.92)
Return to OR
2.10%
2.10%
1.60%
0.541
Readmission
7.20%
6.40%
6.00%
0.304
30-day mortality rate
4.20%
3.70%
5.20%
0.08
aModel adjusted for race, hypertension medication, cancer, bleeding disorders, transfusion within 72 hours before surgery, emergency status, wound infection, anesthesia type (general), body mass index (18.5-25), history of chronic obstructive pulmonary disease, and preoperative levels of creatinine, platelet count, white blood cell count, and hematocrit.