SAN DIEGO – Principles for lip repair are based on size and location of the defect, etiology of the lesions, and patient age and gender, said Dr. Michael A. Keefe.
Surgical goals of lip reconstruction are to cover the skin and oral lining, leave a semblance of a vermilion and an adequate stomal diameter, make sure sensation is intact, and ensure that the patient has a competent oral sphincter. "The vermilion is the most visible component of the lips, and it’s also the sensory unit of the lip," Dr. Keefe said at a meeting on superficial anatomy and cutaneous surgery. The meeting was sponsored by the University of California, San Diego, School of Medicine and the Scripps Clinic.

Dr. Michael A. Keefe
"Scars are very well hidden at the vermilion-cutaneous border. If you have to cross the vermilion-cutaneous junction, cross at 90 degrees."
Lower Lip
The lower vermilion is the most affected target of solar radiation injury. In cases of premalignant lesions such as actinic cheilitis or leukoplakia, Dr. Keefe, a plastic surgeon with the division of head and neck surgery at Sharp Rees-Stealy Medical Group in San Diego, said he often performs a total vermilionectomy (lip shave). This involves resection from the white roll to the contact area with opposite lip. "Primary closure is possible," he said. "You can get tension and dehiscence and flattening of the lip, but generally it heals up pretty well. An option for vermilion reconstruction of larger defects is the buccal mucosal advancement flap, which involves elevating the mucosa deep to salivary glands and superficial to the orbicularis oris muscle."
An advantage of treating the lower lip is that there is increased soft tissue laxity and there is no Cupid’s bow, philtrum, or nose, "so it’s nice that there are no dominant central structures," he said. "The downside is that you have to be mindful of the effect of gravity on the repair, so there is a greater need for tone to prevent drooling and incompetence."
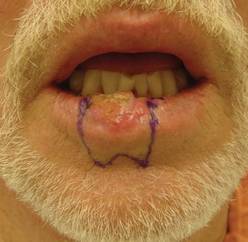 Photos courtesy Dr. Michael Keefe
Photos courtesy Dr. Michael Keefe
This man had a primary repair of a 1/3 lower lip defect with a "W-plasty" of the lower lip so as not to cross the labiomental groove.
He recommends a staged approach based on the extent of the defect and the age of the patient. For small defects (those less than one-third of the lip size) he uses primary closure. Options for medium defects (those that involve one-third to two-thirds of the lip size) include the Estlander flap, the Abbe flap, Bernard Burow’s procedure, the Karapandzic flap, and the stairstep repair, while the options for large defects (those that involve more than two-thirds of the lip size) include Bernard Burow’s procedure, the Karapandzic flap, and the free flap. "You have a lot of tools, depending on what you feel comfortable with," Dr. Keefe said.
Upper Lip
Cancerous tumors of the upper lip are less common, "but there are some unique structures to pay attention to, including the nose, columella, Cupid’s bow, and the philtrum," he said. "In men there’s a hair-bearing skin issue, but scars can be disguised in a mustache."
The aesthetic subunits to keep in mind, he continued, are the medial subunit, which is one-half of the philtrum, and the lateral subunit, which consists of the philtral column, the nostril sill, the alar base, and the nasolabial crease. Primary closure is used for upper lip defects that involve less than one-third of the lip size. "You can make some perialar crescentic skin excisions, which can help advance things," Dr. Keefe said.
For centrally located medium-sized defects of the upper lip, he often uses primary closure with perialar crescentic skin excisions. "If it’s greater than one-half of the lip size, you can add an Abbe flap," he said. "That’s nice because that recreates the philtrum area."
 Photos courtesy Dr. Michael Keefe
Photos courtesy Dr. Michael Keefe
The same man, post-lip repair.
For medially located medium-sized defects of the upper lip, "you can use the Abbe flap if the commissure is not involved and the Estlander flap if the commissure is involved."
Options for cases with large defects and adequate cheek tissue, he said, include the reverse Karapandzic flap, the reverse fan flap, inverted Bernard Burow’s procedure, superiorly based cheek flaps, and the bilateral levator anguli oris flap combined with the Abbe flap. Options for cases with inadequate cheek tissue include the distal pedicle flap and the free flap.
Repair Risks
A lot of these patients have medical problems," he said. "When you do your first injection to resect the tumor or put the lip back together, make sure you don’t cause a myocardial infarction. Generally you should be comfortable with patients who have an INR [International Normalized Ratio] of 2.5 and below."