Acute kidney injury is a serious adverse effect of cardiac surgery, and contrast-induced nephropathy due to coronary angiography has been suggested as a potentially important component. However, the results of a retrospective study of more than 2,500 patients showed that acute kidney injury is significantly higher only in those patients who have combined cardiac surgery within 24 hours of catheterization.
The study by Dr. Giovanni Mariscalco of the Varese (Italy) University Hospital, and his colleagues assessed all consecutive patients undergoing cardiac surgery at the hospital between Jan. 1, 2005, and Dec. 31, 2011. The operations performed were isolated coronary artery bypass grafting (CABG), valve surgery with or without concomitant CABG, and proximal aortic procedures. After exclusion of patients who did not undergo cardiopulmonary bypass, a known major cause of acute kidney injury (AKI), and those who died during the procedure, a total of 2,504 patients remained. These patients had a mean age of 68.4 years and consisted mostly of men (67.3%), according to the report in the April issue of the International Journal of Cardiology.
 Courtesy Wikimedia Commons/ Pantaleo et al. BMC Cancer 2012.12:231/Creative Commons License
Courtesy Wikimedia Commons/ Pantaleo et al. BMC Cancer 2012.12:231/Creative Commons License
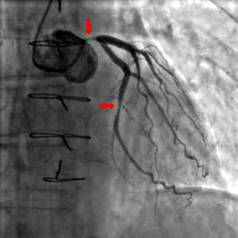
Coronary angiography showing critical sub-total occlusion of the common trunk of the left coronary artery and circumflex artery.
The primary endpoint of the study was the effect of timing between cardiac catheterization and surgery on the development of AKI. Postoperative AKI was defined by the consensus RIFLE criteria (risk, injury, failure, loss of function, and end-stage renal disease), using the maximal change in serum creatinine and the estimated glomerular filtration rate during the first 7 days after surgery, compared with baseline values collected the day before surgery or immediately before surgery when cardiac catheterization was performed on the same day as the operation.
The researchers defined AKI as a 50% increase in the postoperative serum creatinine over baseline. Propensity analysis was used to match patients, who were then assessed both pre- and postmatch.
The overall incidence of AKI after surgery was 9.2% (230/2,504 patients). A breakdown by procedure showed that AKI occurred in 7.7% of isolated CABG patients, 12.2% of isolated valve patients, 9.5% of combined-procedure patients, and 9.5% of the proximal aorta surgery patients (Int. J. Cardiol. 2014;173:46-54).
As has been seen in previous studies, AKI was associated with patient-specific pre- and perioperative variables, including increased patient age, added comorbidities, longer cardiopulmonary bypass (CPB) times, higher rates of combined procedures, and the use of intra-aortic balloon pumps.