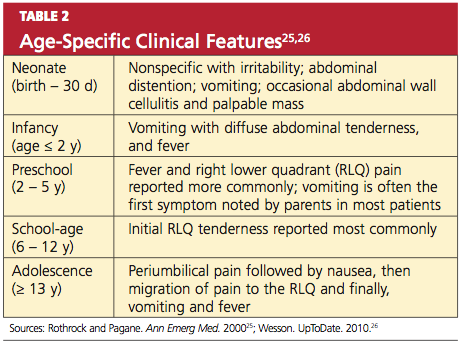
According to results from other studies, unfortunately, this progression of symptoms is not often present in pediatric patients.17 The somatic RLQ pain is continuous and more severe than is the early visceral periumbilical pain.1 Since the anatomic position of the appendix can vary, a number of patients do not necessarily present with pain in the RLQ but elsewhere.24 Certain clinical findings appear to be relatively age-dependent (see Table 225,26).
Classic findings in the adult diagnosed with appendicitis, as described by Becker et al,27 begin with periumbilical pain, then nausea, followed by migration of the pain to the RLQ, then vomiting and fever. Abdominal pain and anorexia are the most common presenting symptoms.20 Nausea and vomiting that begin after the onset of abdominal pain are typical; in isolation, however, these manifestations have weak diagnostic predictability for appendicitis.28 In adults, if nausea and vomiting precede abdominal pain, consideration should be given to a diagnosis of gastroenteritis rather than appendicitis.29
Among patients who are pregnant or elderly, RLQ pain remains a significant historical finding.30 In the pregnant woman, a diagnosis of appendicitis is often overlooked because of the discomforts common to pregnancy and the expanding gravid uterus.31 Elderly patients often present with vague or atypical symptoms, such as mild pain.20 In these patient populations, the diagnosis of appendicitis is often delayed.
In addition to obtaining a thorough history of the presentation of pain, it is important to conduct a complete review of the gastrointestinal, genitourinary, pulmonary, musculoskeletal, neurologic, and reproductive systems for possible alternate etiologies.
Physical Examination
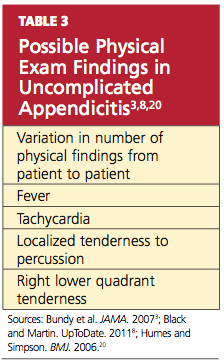
The number of physical findings varies among patients who present with appendicitis3,8,20 (see Table 33,8,20). A thorough physical examination is thus required to help the clinician exclude other diseases and establish the diagnosis of appendicitis. It is important to tailor the exam according to the patient’s age and developmental stage.19
The cooperation of children undergoing the physical examination for appendicitis may vary. It may be helpful to instruct a young child to “show me with your finger where it hurts the most.”3 However, Bundy et al3 report that the presence of RLQ tenderness on palpation is of minimal value in children; rather, fever is the single most useful sign among pediatric patients and conversely, its absence reduces the risk.
Tachycardia is associated with risk for rupture.16,20 In the elderly patient, fever (> 38°C) is also strongly correlated with an increased risk for rupture.30
To alleviate pain, a patient with appendicitis may maintain the hips and knees in a slightly flexed position. While asking distracting questions, the examiner should observe the patient’s facial expressions to detect involuntary guarding.3 RLQ tenderness to percussion is often positive.
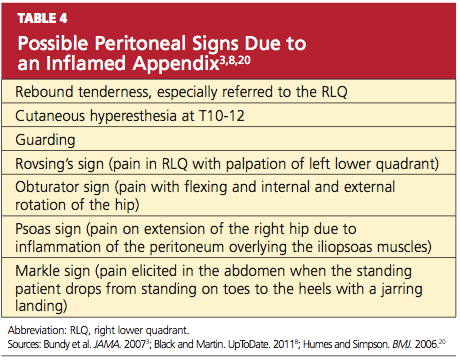
The patient may experience tenderness on palpation of the posterior abdominal wall (K sign) or right-side flank tenderness.24 Increased pain with coughing (Dunphy’s sign) or firm percussion of the heel (the heel jar test) may be elicited.8,25 A number of additional peritoneal signs, resulting from an inflamed appendix, may occur (see Table 43,8,20), but examination techniques that elicit these signs should be minimized so as to not cause the patient any unnecessary pain.
Depending on the location of the appendix, rectal and vaginal exams may yield normal findings or may elicit tenderness.32 The rectal examination should be performed with considerable care, using the smallest digit possible for an adequate assessment, especially in the younger patient.33
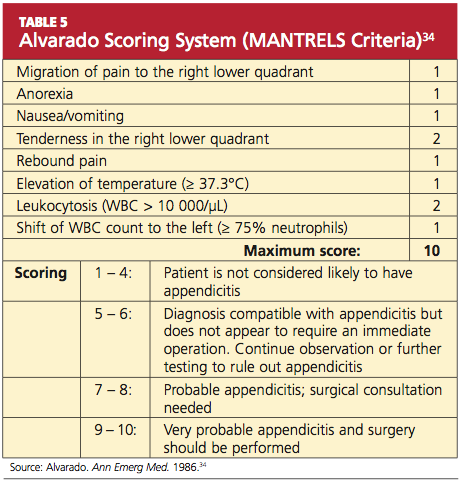
Several scoring systems have been designed for adults and children with suspected appendicitis, using findings from the history, the physical exam, and laboratory testing (see Table 5,34 for example). Despite their protocol-based approach, the scoring systems have yielded mixed results in clinical practice,34-36 and there is no scoring system for evaluation of the pregnant patient.37 Neither has there been any recommendation for or endorsement of a diagnostic guideline from any medical or professional organization.38 Thus, clinical gestalt is usually relied upon instead.
Conditions to Rule Out
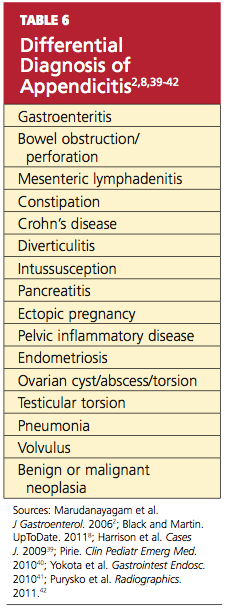
The patient with abdominal pain and suspected appendicitis should be evaluated for other causes during the physical examination (see Table 62,8,39-42). In addition to investigation for other abdominal etiologies, auscultation to the heart and lungs and an assessment of the peripheral vasculature are imperative. Auscultation of the lungs is important to rule out a right lower lobe pneumonia that may generate referred pain to the RLQ due to a shared T9 dermatome distribution.20,25
In males, the patient with abdominal pain should be assessed for a testicular etiology, and a pelvic examination is indicated in any female with abdominal pain, to rule out a gynecologic origin.1,3 In the infant with suspected appendicitis, a diagnosis of Hirschsprung’s disease (a congenital obstruction of the colon) should also be considered.17