Celiac disease (CD), also known as gluten-sensitive enteropathy or celiac sprue, is an endocrine disorder whose effects are triggered by the ingestion of gluten—the principle storage protein in wheat, rye, and barley.1-3 CD inflicts damage to the mucosa of the small intestine and subsequently to systemic organ tissues. CD can affect any organ in the body.1 The responsible genetic factors are the human leukocyte antigens, HLA -DQ2 and -DQ8, which are present in 40% of the general population but are found in nearly 100% of patients with CD.1,3,4
Though previously considered uncommon, CD has been estimated to affect more than 1% of the general population worldwide.1,4,5 Currently, CD is most reliably identified by positive serum antibodies, specifically immunoglobulin A (IgA) anti-tissue transglutaminase (tTG) and IgA antiendomysial (EMA) antibodies,6 and by a finding of villous atrophy of the intestinal lining on biopsy. The spectrum of presentations of CD is broad, including the “typical” intestinal features of diarrhea, bloating, abdominal pain, and weight loss; or common “atypical” extraintestinal manifestations, such as anemia, osteoporosis, infertility, and neurologic disturbances (eg, peripheral neuropathy7).8 See Table 1.8,9
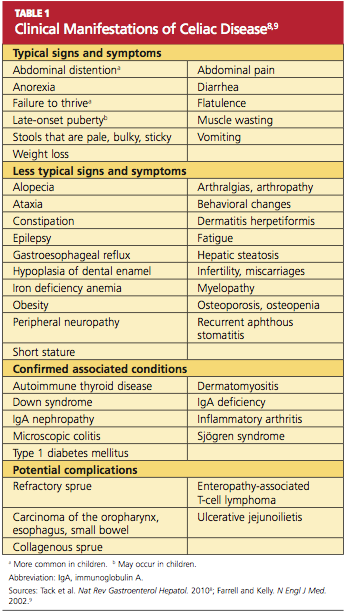
Prevalence of CD is greater among those with a family history of CD; with autoimmune diseases, especially type 1 diabetes mellitus (T1DM) and thyroiditis; and with certain genetic disorders (ie, Down, Turner, and Williams syndromes).8-15 Because atypical features dominate in older children and adults, many cases escape diagnosis, and patients may be exposed to serious long-term complications, such as infertility and cancer.1
CD is a lifelong condition, necessitating the complete exclusion of gluten-containing products from the diet. In the US food industry, gluten is used in numerous food applications, complicating the patient education and lifestyle changes needed to implement and maintain a gluten-free diet (GFD). However, if a GFD is not strictly followed, the patient’s quality of life can be seriously impaired.1,4,5
AWARENESS ESSENTIAL IN PRIMARY CARE
For the primary care provider (PCP), there is no shortage of patients with gastrointestinal (GI) disorders, thyroid disease, diabetes, anemia, fatigue, or dysmenorrhea; additionally, PCPs regularly treat patients for a number of associated disorders, including anxiety, irritability, and attention deficit. Yet how likely are PCPs to screen patients with these symptoms for CD? And how many patients with CD never receive a diagnosis of the disorder?
In fact, it has been estimated that more than 90% of persons affected by CD are currently undiagnosed.1,4 In one study involving mass screening of 1,000 children ages 2 to 18, it was determined that almost 90% of celiac-positive children had not previously been diagnosed.5 Similarly, in a cohort of 976 adults (median age, 54.3), the diagnostic rate for CD was initially low at 0.27 cases per thousand visits but increased to 11.6 cases per thousand visits after implementation of active screening.4 Based on these data, it has been estimated that more than 2.7 million Americans unknowingly carry this potentially life-threatening genetic disease.1,4,16
Given the potential patient population with undetected, untreated CD, some researchers consider the disorder one of the most common lifelong diseases in the US.1,8,16 CD is closely associated with T1DM and autoimmune thyroiditis, with cross- prevalence at 11% and 6.7%, respectively.8,12,17 The close association between T1DM and CD led the American Diabetes Association18 to amend guidelines in 2009, suggesting screening for CD in all patients newly diagnosed with T1DM.
PATIENT PRESENTATION: ADULTS VERSUS CHILDREN
Most infants and young children with CD present with the typical or “classic” triad of signs: short stature, failure to thrive, and diarrhea; in individual patients, however, the impact of genetics and exposure to gluten over time can cause considerable variation in patient presentation. As patients with undiagnosed CD age, they may present quite differently or even revert to a latent stage and become asymptomatic.19,20
In two separate reviews, it was noted that classic symptoms of CD are not evident in a majority of older children and adults; instead, anemia and fatigue were the predominating symptoms.12,20An important note: The patient with no symptoms or atypical signs of CD may still be experiencing significant damage, inflicted by gluten-induced antibodies, to the intestinal lining and/or mucosal linings in other organ systems—perhaps for years before the disease becomes evident.20
Clinical Findings Differ With Age, Gender
Historically, CD was considered a pediatric syndrome; however, a diagnosis of CD has become increasingly common among older children and adults, especially elderly patients, although symptoms in the latter group are subtle.21-23 Recent, active CD is being diagnosed among men older than 55 more commonly than in women of this age-group; women are generally younger at diagnosis but have experienced symptoms longer.22,23 This later onset in men suggests that antibody seropositivity and the associated active disease may be triggered later in life.8,22