DIAGNOSTIC IMAGING
In mTBI management, the sole purpose of diagnostic imaging is to rule out a more severe structural injury, such as intracranial hemorrhage or hematoma. Symptoms commonly associated with mTBI, such as nausea, vomiting, headache, and visual disturbances, are also cardinal signs of a mass effect resulting from both subdural and epidural hematomas. When these symptoms occur in the acute phase of mTBI management, immediate CT without contrast is imperative to rule out skull fracture and intracranial hemorrhage. Note: Negative imaging test results in the presence of mTBI symptoms do not rule out mTBI, a functional injury; they only confirm that no structural pathology exists.1
Clinicians must also be aware that because a subdural hematoma accumulates slowly, positive findings may not be evident on CT or MRI for seven to 14 days after the initial injury. Thus, the sudden return or worsening of mTBI symptoms that were previously resolved or stable warrants evaluation for a slower (and more commonly fatal) chronic subdural hematoma.1 In this emergent case, CT without IV contrast should be performed first to rule out acute hemorrhage or any mass effect. However, because of the lysing effect of clotted blood, CT with IV contrast or MRI is needed to definitively determine dural and gray-matter reactions to an occult bleed.27
At this time, there is no gold standard among imaging techniques to capture the functional disturbances often noted with sport-related mTBI. However, in one recent study of functional MRI (fMRI) use following sport-related mTBI, athletes with evidence of hyperactivation on their initial post-mTBI scan took longer to recover, based on symptom presentation and neurocognitive testing.28 Though currently used for research purposes, fMRI appears to demonstrate measurable metabolic changes in the brain even after symptoms have been resolved. This promising modality may soon provide helpful neurophysiologic data for the clinical assessment and management of sport-related mTBI.
SYMPTOM SURVEILLANCE
The second component of clinical management of mTBI is the follow-up and surveillance of symptoms and neurologic limitations over time. This is essential for making clinical decisions, including the appropriate time to return the athlete safely to sports or work, so as to avoid further injury.
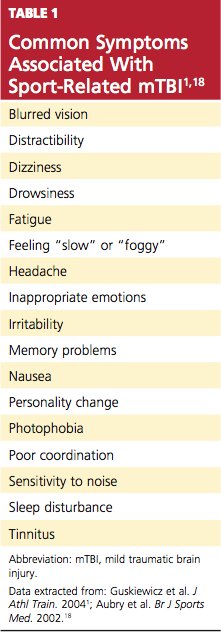
While the acute component of mTBI management relies on the objective nature of physical examination and neuroimaging, follow-up and surveillance are heavily dependent on the subjective symptoms (see Table 11,18), particularly when physical examination and neuroimaging findings are unremarkable.27,29 Therefore, sensitive and specific clinical tools are needed to accurately assess the various elements of cognition and psychological functioning that are most commonly impaired by mTBI.30
COGNITIVE ASSESSMENT
The metabolic changes that occur after cerebral injury have been shown to cause temporary deficits in normal cognition.23,31 Within the first 24 hours of injury, mild to moderate cognitive impairment is noted across all domains, with the greatest deficits occurring in global functioning, memory acquisition, and delayed memory. Deficits in these areas have been shown to resolve within seven to 10 days following the initial injury.31 It is helpful for these cognitive domains to have been clinically evaluated before injury (baseline), as postinjury evaluation can more effectively detect the extent of debilitation caused by mTBI; subsequent reevaluations can be used to monitor the rate of recovery.
Neuropsychological testing has been studied extensively to determine its value and use in the assessment of mTBI.18,32 Currently, two types of testing are used. Traditional neuropsychological testing comprises a battery of pencil-and-paper exercises administered and interpreted by a psychologist to evaluate cognition and identify areas of deficit following mTBI.33 Although these tests produce a wealth of data, they are expensive, they may require a referral, and administering them can take longer than four hours.
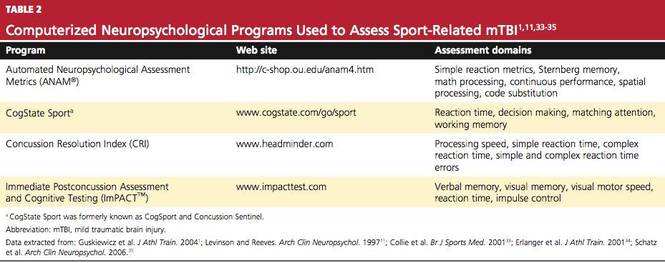
The newest form of neuropsychological testing involves computer-based protocols. Though not yet fully validated, these tools require less time to administer than traditional testing and are commonly used in the sports medicine community (see Table 21,11,33-35 ). Computer-based testing, which may be conducted in the school’s computer lab, has the potential to make preseason baseline testing feasible for large numbers of athletes. Other advantages are ease of administration, a time requirement of about 30 minutes, and the availability of multiple versions to control for the effects of practice.1,23
Two approaches have been suggested for effective use of neuropsychological testing in both components of mTBI management1,30:
First, perform baseline testing at the start of the athletic season, before exposure to injury (possibly within the preparticipation physical), then retest the injured athlete once he or she reports being asymptomatic. Return to play may be considered once the injured athlete scores at or above baseline testing.