Winston Liaw, MD Sarah Coleman, MD Andrew Bazemore, MD, MPH Mark K. Huntington, MD, PhD Fairfax Family Practice Residency Program, Virginia Commonwealth University (Drs. Liaw, Coleman, and Bazemore); The Robert Graham Center, American Academy of Family Physicians, Washington, DC (Dr. Bazemore); Sioux Falls Family Medicine Residency Program and University of South Dakota Sanford School of Medicine (Dr. Huntington) mark.huntington@usd.edu
The authors reported no potential conflict of interest relevant to this article.
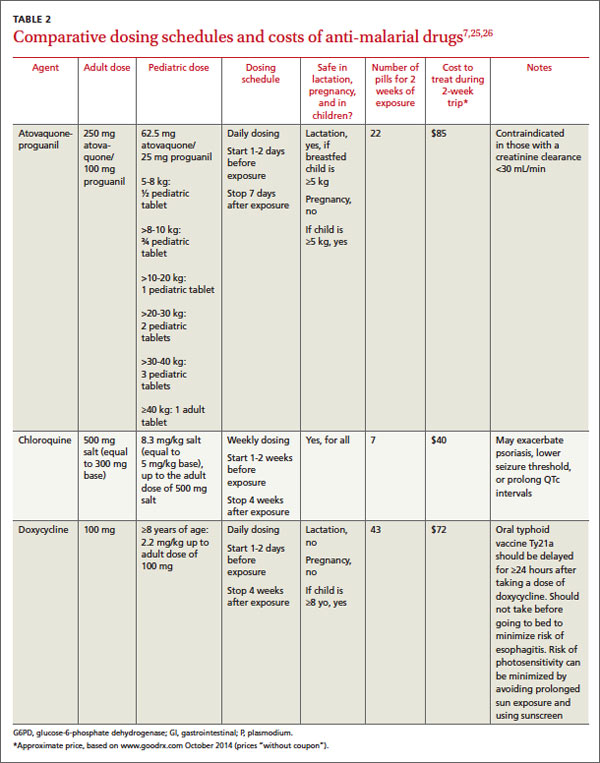
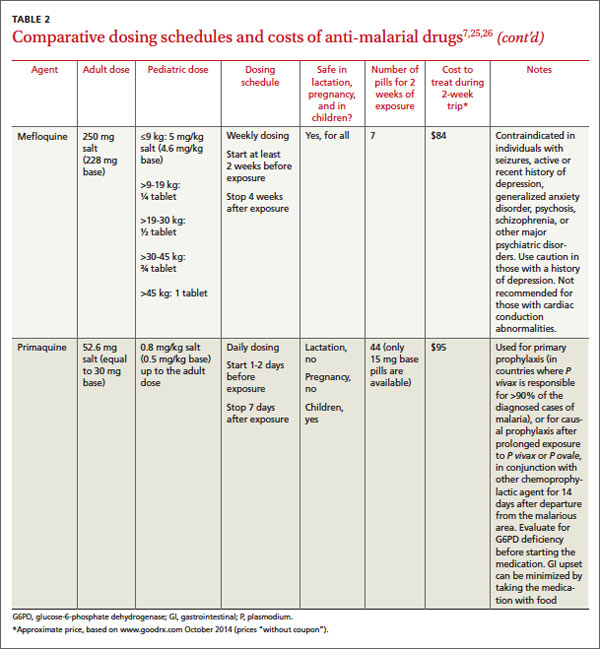
Cost. For a 2-week exposure period, chloroquine is the least expensive medication (although regions in which it is recommended are limited due to resistance) (TABLE 27,25,26).
Ask about accommodations Since Anopheles mosquitoes feed between dusk and dawn, inquiring about accommodations can further clarify a patient’s malaria risk. Staying in air-conditioned housing (implying that the interior can be sealed) or that has screened windows can reduce exposure to mosquitoes, although data are lacking regarding whether the latter practice reduces the incidence of malaria transmission28 (SOR: C).
Share decision making After considering the key factors determining a patient’s level of risk, you may decide to recommend no specific interventions, to advise insect avoidance measures only, to combine insect avoidance with chemoprophylaxis, or to caution against traveling to a malaria-endemic region. The patient’s contribution to the final decision includes personal preferences, values, and risk tolerance—particularly when comorbidities are involved.
WHEN PREVENTIVE MEASURES FAIL Approximately 0.2% of travelers to malaria-endemic regions will become infected, despite proper pre-travel counseling and prophylaxis.29 In the United States, malaria is often misdiagnosed or improperly treated.30 The time from initial presentation to correct diagnosis of malaria has been reported as an astonishingly high 4 to 8.5 days, depending on the population.31,32
A high index of suspicion is needed and will ensure timely care when any febrile traveler returns from a malaria-endemic area.33 Be sure to advise patients to seek medical attention if they are feverish upon returning home.
Once suspected, the diagnosis of malaria can be readily confirmed through the use of antibody-, nucleic acid-, or microscopy-based techniques (the latter to directly visualize Plasmodium species in blood smears).
Although malaria chemoprophylaxis is relatively straightforward, malaria treatment—especially in cases of chemoprophylaxis failures—may not be, and the topic is beyond the scope of this article. For guidance on treating malaria, consult a knowledgeable physician or contact the CDC at www.cdc.gov/malaria/, or at (855) 856-4713 (weekdays, 9 am to 5 pm EST) or (770) 488-7100 (weekends or after normal business hours; ask for the Malaria Branch clinician on call).
CORRESPONDENCE Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; mark.huntington@usd.edu