Syril Keena T. Que, MD; Taylor DeFelice, MD, MPH; Farah R. Abdulla, MD; David Cassarino, MD; Rishi R. Patel, MD
Dr. Que was from and Drs. DeFelice and Patel are from the New York University School of Medicine, New York. Drs. DeFelice and Patel are from the Ronald O. Perelman Department of Dermatology. Dr. Que currently is from the Department of Dermatology, University of Connecticut, Farmington. Drs. Abdulla and Cassarino are from Kaiser Permanente Fontana Medical Center, California. Dr. Abdulla is from the Department of Dermatology and Dr. Cassarino is from the Department of Pathology.
The authors report no conflict of interest.
Correspondence: Rishi R. Patel, MD, Ronald O. Perelman Department of Dermatology, New York University School of Medicine, 530 1st Ave, Ste 7J, New York, NY 10016 (rishi.patel@nyumc.org).
Figure 4. Purple papules and hyperkeratotic hyperpigmented plaques on the medial aspect of the right leg.
If similar presentations of KS are identified, studies will need to be done to uncover the specific risk factors involved. Human herpesvirus 8 is not sufficient for the development of KS on its own, as oncogenesis of KS requires immunodeficiency or an additional environmental factor such as diabetes mellitus.5 Through impaired microvascular circulation and the release of hypoxia-inducible factor 1a, diabetes can promote KS-herpesvirus replication. Therefore, the risk for KS is increased in individuals with diabetes regardless of a negative history of immunodeficiency, which may have been the case in patient 2.
Our cases suggest that chronic venous insufficiency may be another factor that predisposes immunocompetent individuals to KS. Chronic venous insufficiency can cause hypoxia, promoting the release of cytokines and angiogenic factors responsible for the formation of vascular tumors such as KS.6 Once present, KS can worsen preexisting stasis dermatitis by compressing the external lymphatics and exacerbating lymphedema.7 Stasis dermatitis and KS may be part of a self-perpetuating cycle that involves obstruction due to secondary lymphadenopathy, the development of lymphedema, and the release of cytokines and growth factors that lead to further vascular proliferation.8
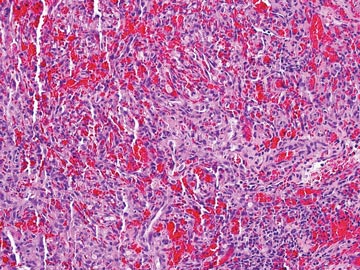
Figure 5. A cellular dermal vascular proliferation associated with slitlike vessels, dermal fibrosis, and marked cellularity with nuclear atypia (H&E, original magnification ×200).
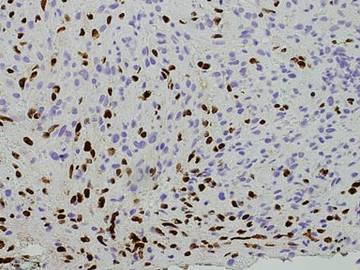
Figure 6. Spindled cells reactive to human herpesvirus 8 immunostain (original magnification ×400).
In summary, we present 2 cases of non–HIV-related KS that may represent an additional clinical variant of KS that mimics and/or arises in chronic venous insufficiency and appears as papules and plaques in elderly patients who are Hispanic, immunocompetent, and HIV negative. We suggest including KS in the differential diagnosis for chronic venous insufficiency, especially in cases with an unusual clinical appearance or course. In these cases, skin biopsy with HHV-8 testing may be warranted.
Acknowledgment
The authors would like to acknowledge William Putnam, BFA, New York, New York, for his assistance with the figures.