Bart D. Wilkison, MD; Leonard C. Sperling, MD; Anne P. Spillane, MD; Jon H. Meyerle, MD
Dr. Wilkison is from Brooke Army Medical Center, San Antonio, Texas. Drs. Sperling and Meyerle are from the Department of Dermatology, F. Edward Hebert School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland. Dr. Spillane is from Kimbrough Ambulatory Care Clinic, Fort Meade, Maryland.
The authors report no conflict of interest.
The opinions expressed in this article are solely those of the authors and do not necessarily reflect the official policy or position of the US Army or the US Department of Defense.
Correspondence: Jon H. Meyerle, MD, Department of Dermatology, F. Edward Hebert School of Medicine, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Rd, Bethesda, MD 20814 (jon.meyerle@usuhs.edu).
Figure 2. Adding 10% potassium hydroxide solution to skin samples.
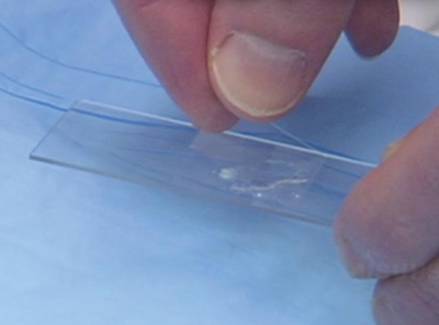
Figure 3. Placing the slide coverslip.
Figure 4. Applying gentle heat to the potassium hydroxide preparations.
Microscopic Examination
Prior to examining the slides under the microscope, students may complete a self-guided tutorial (eg, digital or paper slide show) on the various features seen through the microscope that are indicative of dermatophytes, including branching hyphae and yeast buds. They also should be educated about the common appearance of artifacts that may resemble hyphae. Once the students have completed the tutorial, they may proceed to microscopic examination.
While the students are viewing their slides under the microscope, we find it helpful to have at least 1 experienced faculty member for every group of 10 students. This instructor should encourage the students to lower the microscope condenser all the way to facilitate better observation. Students should start with low power (×4 or red band) and scan for areas that are rich in skin scale. Once a collection of scale is found, the student can switch to higher power (×10 or yellow band) and start scanning for hyphae. Students should be reminded to search for filamentous and branching tubes that are refractile. The term refractile may be confusing to some students, so we explain that shifting the focus up or down will show the hyphae to change in brightness and may reveal a greenish tint. Another helpful indicator to point out is the feature that hyphae will cross the border of epidermal skin cells, whereas artifacts will not (Figure 5). Once the students have identified evidence of a dermatophyte infection, they must call the instructor to their station to verify the presence of hyphae or yeast buds, which helps confirm their understanding of the procedure. Once the student accurately identifies these items, the session is complete.
Figure 5. Example of hyphum crossing epithelial cell borders. Figure 5. Example of hyphum crossing epithelial cell borders.
Figure 5. Example of hyphum crossing epithelial cell borders.
Comment
The use of a KOH preparation is a fast, simple, accurate, and cost-effective way to diagnose superficial fungal infections; however, because of insufficient familiarity with this tool, the technique often is replaced by initiation of empiric antifungal therapy in patients with suspected dermatophytosis. This empiric treatment has the potential to delay appropriate diagnosis and treatment (eg, in a patient with nummular dermatitis, which can clinically mimic tinea corporis). One way to encourage the use of the KOH preparation in the primary care and dermatologic setting is to educate large groups of next-generation physicians while in medical training. This article describes a teaching technique that allows for long-term storage of positive skin samples and a detailed description of the pedagogy used to train and educate a large group of students in a relatively short period of time.
All KOH preparations fall under the US federal government’s Clinical Laboratory Improvement Amendments and require proficiency testing.9 Although the teaching method presented here is designed for teaching medical students, it may be utilized to educate or refamiliarize experienced physicians with the procedure in an effort to improve proficiency in point-of-care testing programs used in many health care systems to comply with the Clinical Laboratories Improvement Amendments. Future analyses could assess whether the method described here improves provider performance on such proficiency measures and whether it ultimately helps ensure quality patient care.