Status Report From the American Acne & Rosacea Society on Medical Management of Acne in Adult Women, Part 1: Overview, Clinical Characteristics, and Laboratory Evaluation
Dr. Del Rosso is from Touro University College of Osteopathic Medicine, Henderson, Nevada, and Las Vegas Dermatology, Nevada. Dr. Harper is in private practice, Birmingham, Alabama. Dr. Graber is in private practice, Boston, Massachusetts. Dr. Thiboutot is from Penn State University Medical Center, Hershey. Dr. Silverberg is from the Department of Dermatology, Mount Sinai St. Luke’s-Roosevelt and Beth Israel Medical Center of the Icahn School of Medicine at Mount Sinai, New York, New York. Drs. D.Z. and L.F. Eichenfield are from the University of California, San Diego School of Medicine. Dr. L.F. Eichenfield also is from Rady Children’s Hospital, San Diego, California. Dr. Del Rosso is an advisory board member, consultant, and/or speaker for Allergan, Inc; Aqua Pharmaceuticals; Bayer Health Care Pharmaceuticals; Dermira, Inc; Ferndale Laboratories, Inc; Galderma Laboratories, LP; Mimetica; Promius Pharma; Ranbaxy Laboratories Limited; Sebacia; Suneva Medical, Inc; Unilever; and Valeant Pharmaceuticals International, Inc. He also is a researcher for Allergan, Inc; Ranbaxy Laboratories Limited; Sebacia; and Suneva Medical, Inc. Drs. Harper, Graber, D.Z. Eichenfield, and L.F. Eichenfield report no conflict of interest. Dr. Thiboutot is a consultant for and has received research grants from Allergan, Inc, and Galderma Laboratories, LP. Dr. Silverberg has been an investigator for Allergan, Inc, as well as an advisory board member for Galderma Laboratories, LP, and Johnson & Johnson Consumer Inc.
This article is an educational initiative of the American Acne & Rosacea Society (AARS) intended to be a general guide to assist the clinician. The content has been developed solely by the authors. There was no input or contribution from industry or any outside agency related to this publication. The content was reviewed and approved by the authors and Board of Directors of the AARS. This article is the first of a 3-part series. The second part will appear next month.
Acne presenting in adult women is commonly encountered in clinical practice. Many affected women have had acne during their teenaged years, have tried several therapies in the past, and are seeking effective treatment. Others are frustrated by the inexplicable emergence of acne as an adult when they never had it as a teenager. Both groups seek an explanation of why they have acne, are often psychosocially affected by its effects on appearance and self-esteem, and all are wanting effective and safe treatment. Clinicians are encouraged to connect favorably with each patient through careful history and physical examination and to consider underlying causes of androgen excess. Practical approaches to examination and laboratory evaluation are discussed.
Acne in adult women is common and may persist beyond the adolescent years or may be late in onset with emergence usually during the early to mid-20s.
Adult women with acne often are frustrated, as they perceive it as a disorder of teenagers and are perplexed by its presence later in life. They often are distressed by unpredictable flares as well as difficulty with covering lesions and associated dyschromia and scarring.
Clinical patterns of acne in adult women are mixed inflammatory and comedonal facial acne or a U-shaped pattern of inflammatory lesions involving the lower face and neck.
Laboratory testing is not considered mandatory in all cases. The clinician is encouraged to carefully evaluate each case and determine if further evaluation to detect a cause of androgen excess is warranted.
References
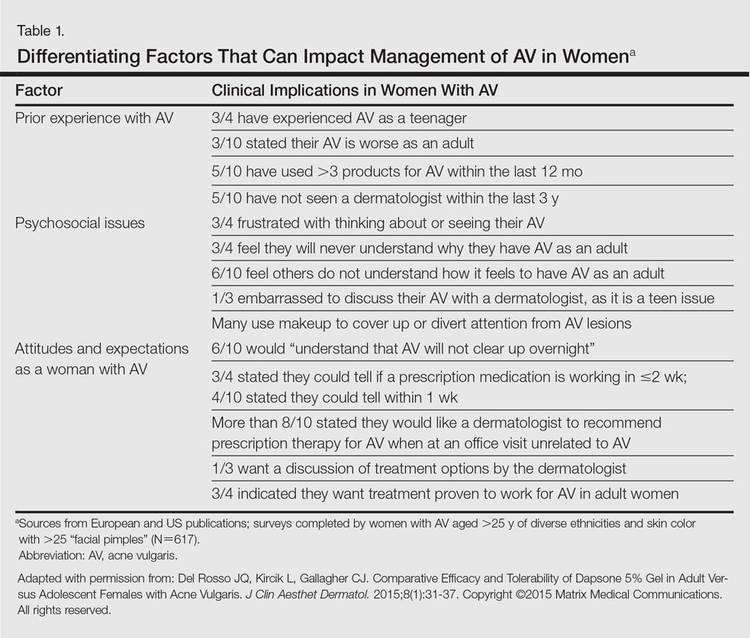
It was not long ago that acne vulgaris (AV) was commonly considered to be a skin disease that affected teenagers with little attention given to preadolescent and postadolescent AV. This perspective has changed, with more attention being given to AV across a broad range of affected age groups, including preadolescent, adolescent, and postadolescent subgroups.1-5 Earlier onset of adrenarche has led to earlier development of AV in many young girls, with a higher range of dehydroepiandrosterone sulfate (DHEAS) levels observed overall in those with AV as compared to a normal age-matched population.3,4 At the other end of the age spectrum, AV is a common phenomenon in adult females, with at least half of women estimated to exhibit some form of AV.1,2,5-8 Based on a large survey of females and males (N=1013), the prevalence of AV in adult females has been reported to be 50.9%, 35.2%, 26.3%, and 15.3% among women aged 20 to 29 years, 30 to 39 years, 40 to 49 years, and 50 years and older, respectively.2 Acne vulgaris that persists beyond adolescence into adulthood is termed persistent acne, or early-onset acne, and the development of AV in women 25 years and older who have not previously been affected by AV has been termed late-onset acne.6,8,9 Publications on the management of AV in adult women have focused primarily on systemic hormonal therapies; however, topical therapies more recently have received greater attention in this subpopulation9-12 and will be discussed in part 2 of this series. Because data on AV in women are limited primarily to involvement of the face and neck region, this article does not address truncal AV unless otherwise specified. Table 1 depicts factors that can influence the management of AV in adult women.
Visible Patterns and Considerations for Clinical Evaluation
Clinical Patterns
Although epidemiologic and demographic data are limited in the subpopulation of women with AV, it is reported that females account for up to 82% of adults with AV, with approximately 75% presenting with AV that is clinically similar to their disease course in adolescence.2,5,13 Among those women with persistent AV, some state that their AV is worse compared to adolescence, while others report it is not as severe. The pattern of AV often is similar to that seen in adolescence, presenting as mixed comedonal and inflammatory papular/pustular lesions diffusely distributed on the face; in other cases, a more selectively distributed U-shaped pattern is noted, characterized predominantly by inflammatory papules and/or nodules involving the lower cheeks and jawline margin, with lesions also commonly noted on the anterior and lateral neck.5,8,9,13-16 A U-shaped pattern is believed to be more common in late-onset AV, often with persistence into the mid-40s.1,15,17 It is important to emphasize the need for additional studies on the demographics and clinical characteristics of AV in adult females, especially correlations between onset, age, and clinical patterns of AV.
An international, prospective, observational study assessed the clinical characteristics of AV in adults (aged ≥25 years) at a dermatology visit for acne (N=374).16 Participants who were under management for their AV showed severity grades of mild (clear/almost clear) in 47.3% of cases. Involvement of multiple facial sites—cheeks, forehead, mandibular region, and temples—was noted in 89.8% of women, often with both inflammatory and comedonal lesions, which is a pattern similar to adolescent AV. Inflammatory lesions alone were observed in 6.4% of women, 17.1% had comedonal AV only, and truncal AV was present in 48.4%.16 Additional well-designed studies are needed to determine if this study reflects an accurate qualitative and quantitative depiction of the spectrum of AV in adult females.
Mandibular Pattern
In the observational study of AV in adults, AV localized to the mandibular area was noted in only 11.2% of participants.16 Women with localized mandibular AV were more likely than women without localized AV to be employed, noted greater daily stress levels, and tended to report more psychologically stressful jobs. Interestingly, the subgroup with mandibular acne alone was much less likely to exhibit a global severity grade of moderate or higher (7.1% vs 50.1%), truncal acne (19.0% vs 51.9%), postinflammatory hyperpigmentation (23.8% vs 51.9%), and erythema (19.0% vs 48.4%), suggesting a unique subset of AV presentation.16
Ethnicity/Skin Color
Women of all ethnicities and skin types may be affected by AV.1,18-20Earlier age of onset of AV has been suggested in white women; however, earlier onset of adrenarche may be more frequent in black girls, which supports an earlier age of onset of AV in this subpopulation.15-17Women with skin of color usually express greater concern with persistent dyschromia at sites where lesions have resolved, and presence of acne scars is a concern among women regardless of skin color, ethnicity, or race.18,20-22