From the Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, Jiangsu, China.
The authors report no conflict of interest.
This article was supported by the China Central Public Welfare Research Foundation (grant 303-05-7059) and the National Natural Science Foundation of China (grant 81472872).
Correspondence: Lin Lin, MD, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12 Jiang-Wang-Miao St, Nanjing, Jiangsu, 210042 China (dr_linlin2011@aliyun.com).
Bloom syndrome, a rare autosomal-recessive disorder, characteristically presents with photosensitivity, telangiectatic facial erythema, and growth deficiency. We present a case of Bloom syndrome with uncommon clinical manifestations including alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. We detected the Bloom syndrome gene, BLM, which is one of the members of the RecQ family of DNA helicases, and found changes in 2 heterozygous nucleotide sites in the patient as well as her father and mother.
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.
Figure 1. Uncommon clinical findings of telangiectatic facial erythema, eyebrow hair loss, and reticular pigmentation on the forehead (A), flat nose (B), alopecia areata (C), and short sharpened distal phalanges that were wider than the length of the fingernails (D) in a 12-year-old Chinese girl with Bloom syndrome that was confirmed on genetic testing.
After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
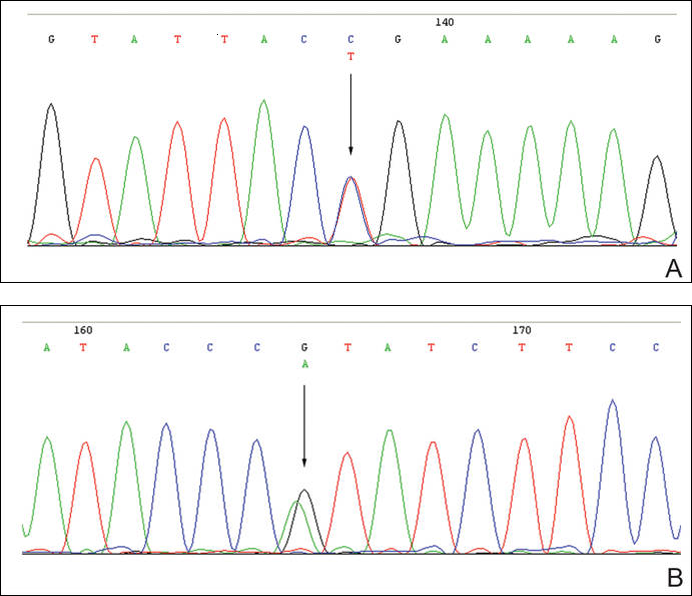
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>Ain exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Figure 2. Changes in 2 heterozygous nucleotide sites: c.2603C>T in exon 13 (A) and c.3961G>A in exon 21 (B) of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A.