Drs. Brooks, Kleinman, and Basile are from the University of Maryland School of Dentistry, Baltimore. Drs. Brooks and Basile are from the Department of Oncology and Diagnostic Sciences, and Dr. Kleinman is from the Department of Periodontics. Dr. Modly is from the Department of Dermatology, University of Maryland School of Medicine, Baltimore.
The authors report no conflict of interest.
Correspondence: John K. Brooks, DDS, Department of Oncology and Diagnostic Sciences, University of Maryland School of Dentistry, Rm 7210, 650 W Baltimore St, Baltimore, MD 21201-1586 (jbrooks@umaryland.edu).
We report the case of a 51-year-old man who presented with an atypical inflammatory response of the gingiva and hard palate that was concomitant with widespread cutaneous psoriasis. The patient had discontinued taking adalimumab 6 months prior to presentation, having achieved satisfactory management of his cutaneous lesions; however, he resumed 2 days prior to presentation due to recurrent disease. A gingival biopsy was consistent with oral psoriasis. At a 2-month follow-up, dramatic resolution of oral involvement was evident and the cutaneous psoriatic plaques were greatly reduced in size. The administration of adalimumab for cutaneous psoriasis may concurrently modulate oral dissemination.
A subset of patients with cutaneous psoriasis may be associated with oral psoriatic outbreaks.
Oral psoriasis presents as an atypical inflammatory response, and histopathologic assessment is recommended for lesional identity.
Use of adalimumab for management of cutaneous psoriasis may demonstrate efficacy for oral psoriasis.
References
Psoriasis is a chronic, relapsing, inflammatory systemic disorder of the skin with an incidence of 2% to 3% and is estimated to affect 125 million individuals worldwide.1 Environmental triggers of disease modulation may include cutaneous microbiota, smoking, alcohol use, drugs (ie, beta-blockers, lithium, antimalarials), stress, and trauma.2 Comorbidities associated with cutaneous lesions include psoriatic arthritis, Crohn disease, type 2 diabetes mellitus, metabolic syndrome, stroke, and cardiovascular disease.3 In some studies, patients with psoriasis also had a 24% to 27% increased propensity for periodontal bone loss versus 10% of controls.4,5
Oral psoriasis is rare and case reports have been preferentially published in dental journals, usually with regard to glossal lesions, leaving gingival and palatal psoriatic involvement infrequently reported in the dermatologic literature.6,7 In fact, oral assessments involving 535 psoriatic patients from a dermatology center only yielded cases of geographic and fissured tongue.8 Another study at a psoriasis clinic found 3.8% (21/547) of patients with geographic tongue, 3.1% (17/547) with buccal mucosal plaques, and only 0.4% (2/547) with palatal lesions.9 To extend the knowledge of oral psoriasis, we provide the clinical and histopathologic findings of a patient with synchronous oral and cutaneous psoriatic lesions that responded well to the administration of adalimumab for management of recurrent cutaneous disease.
Case Report
A 51-year-old man presented to the attending periodontist for comprehensive treatment of multiple quadrants of gingival recession. His medical history was remarkable for psoriasis; Prinzmetal angina, which led to myocardial infarction; and diverticulitis. The cutaneous psoriasis began approximately 18 years prior to the current presentation and was initially managed with various topical therapeutics. At an 11-year follow-up, the patient was experiencing poor lesional control as well as severe pruritus and was prescribed etanercept by a dermatologist. His inconsistent compliance with frequency and dosing failed to achieve satisfactory disease suppression and etanercept was discontinued after approximately 2.5 years. Two years later the patient was switched to adalimumab by a dermatologist, and around this time he had developed psoriatic arthritis of the hands and knees and pitting of the nail plates. The patient elected to discontinue adalimumab usage after 3 years due to successful management of the skin lesions, cost considerations, and his perception that the psoriasis could “remain in remission.” After a 6-month lapse, the patient resumed adalimumab due to cutaneous lesional recurrence (Figure 1A).
Figure 1. Pruritic, erythematous, white, thickened, scaly plaques on the right hand (A). Intensely inflamed and edematous maxillary gingiva (B). Erythematous macules on the hard palate (C).
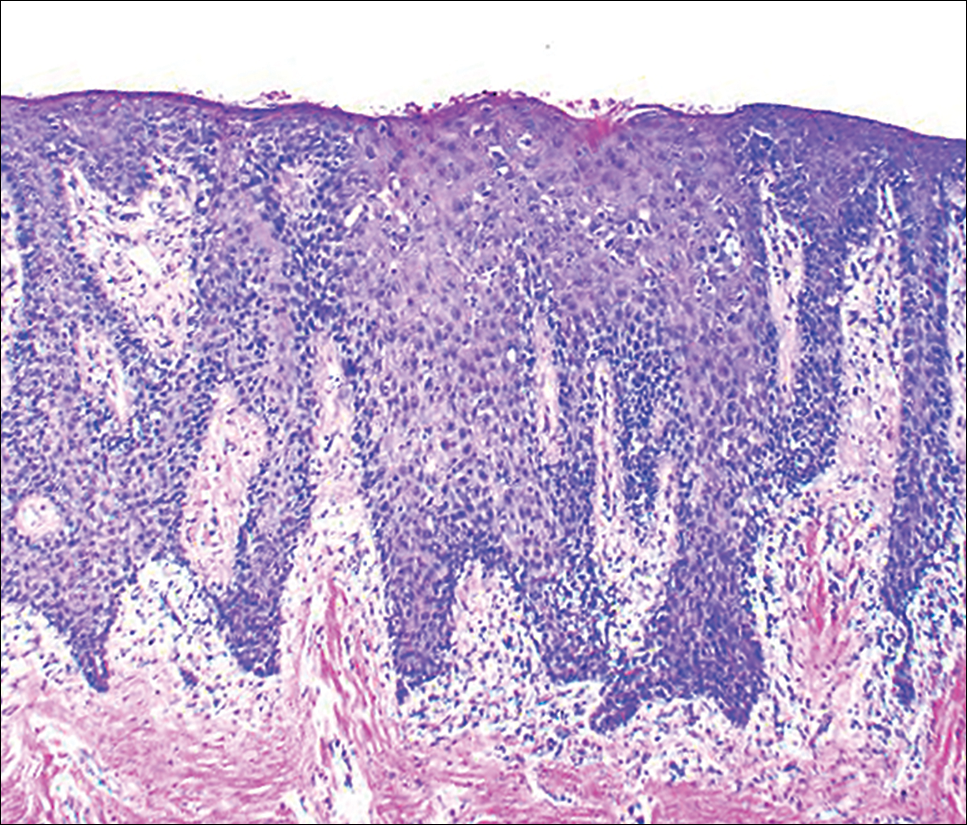
At the current presentation, an oral examination performed 2 days after the reinstitution of adalim-umab revealed generalized severe gingivitis with an atypical inflammatory response that extended from just beyond the mucogingival junction to the marginal gingiva. The gingiva also appeared edematous with a conspicuously granular surface (Figure 1B). The hard palate displayed multiple red macules of varying sizes (Figure 1C). A maxillary gingival biopsy demonstrated hyperkeratosis, parakeratosis, spongiosis, acanthosis, elongation of the rete ridges, numerous collections of neutrophils (Munro microabscesses), and abundant lymphocytes in the subjacent connective tissue (Figure 2). Periodic acid–Schiff staining was negative for fungal hyphae. These features were consistent with oral mucosal psoriasis.
Figure 2. Photomicrograph of maxillary gingival psoriasis demonstrating hyperkeratosis, parakeratosis, acanthosis, elongated rete ridges, Munro microabscesses in the epithelium, and robust lymphocytic infiltrate at the epithelial–connective tissue interface (H&E, original magnification ×10).
At a 2-month follow-up, the biopsy site had healed without incident and without loss of the gingival architecture. There was an almost-complete resolution of the gingival erythema (Figure 3A) and the patient has since noticed a lack of bleeding using floss. Additionally, the red macules on the palate were no longer present (Figure 3B). The cutaneous plaques were greatly reduced in size and the patient experienced a proportionate decline in pruritus. Based on the uneventful surgical biopsy procedure, the patient was advised to undergo gingival grafting and has not returned for periodontal care.
Figure 3. Dramatic reduction in mucosal erythema of the maxillary gingiva (A) and hard palate (B) was seen 2 months after adalimumab treatment was resumed.