Penile squamous cell carcinoma (SCC) with considerable urethral extension is uncommon and difficult to manage. It often is resistant to less invasive and nonsurgical treatments and frequently results in partial or total penectomy, which can lead to cosmetic disfigurement, functional issues, and psychological distress. We report a case of penile SCC in situ with considerable urethral extension with a focus of cells suspicious for moderately well-differentiated and invasive SCC that was treated with Mohs micrographic surgery (MMS).
Mohs micrographic surgery with distal urethrectomy and reconstruction is a valuable treatment technique for cases of SCC involving the glans penis and distal urethra. It offers equivalent or better overall cure rates compared to more radical interventions. Additionally, preservation of the penis with MMS spares patients from considerable physical and psychosocial morbidity. Our case, along with growing body of literature,1-4 calls on dermatologists and urologists to consider MMS as a treatment for penile SCC with or without urethral involvement.
Case Report
A 61-year-old man presented to the dermatology department with a pruritic lesion on the penis that had been present for 6 years. Shave biopsy demonstrated SCC in situ with a focus of cells suspicious for moderately well-differentiated and invasive SCC. Physical examination revealed an ill-defined, 2.2×1.9-cm, pink, eroded plaque involving the tip of the penis and surrounding the external urinary meatus (Figure 1). There was no palpable inguinal lymphadenopathy.
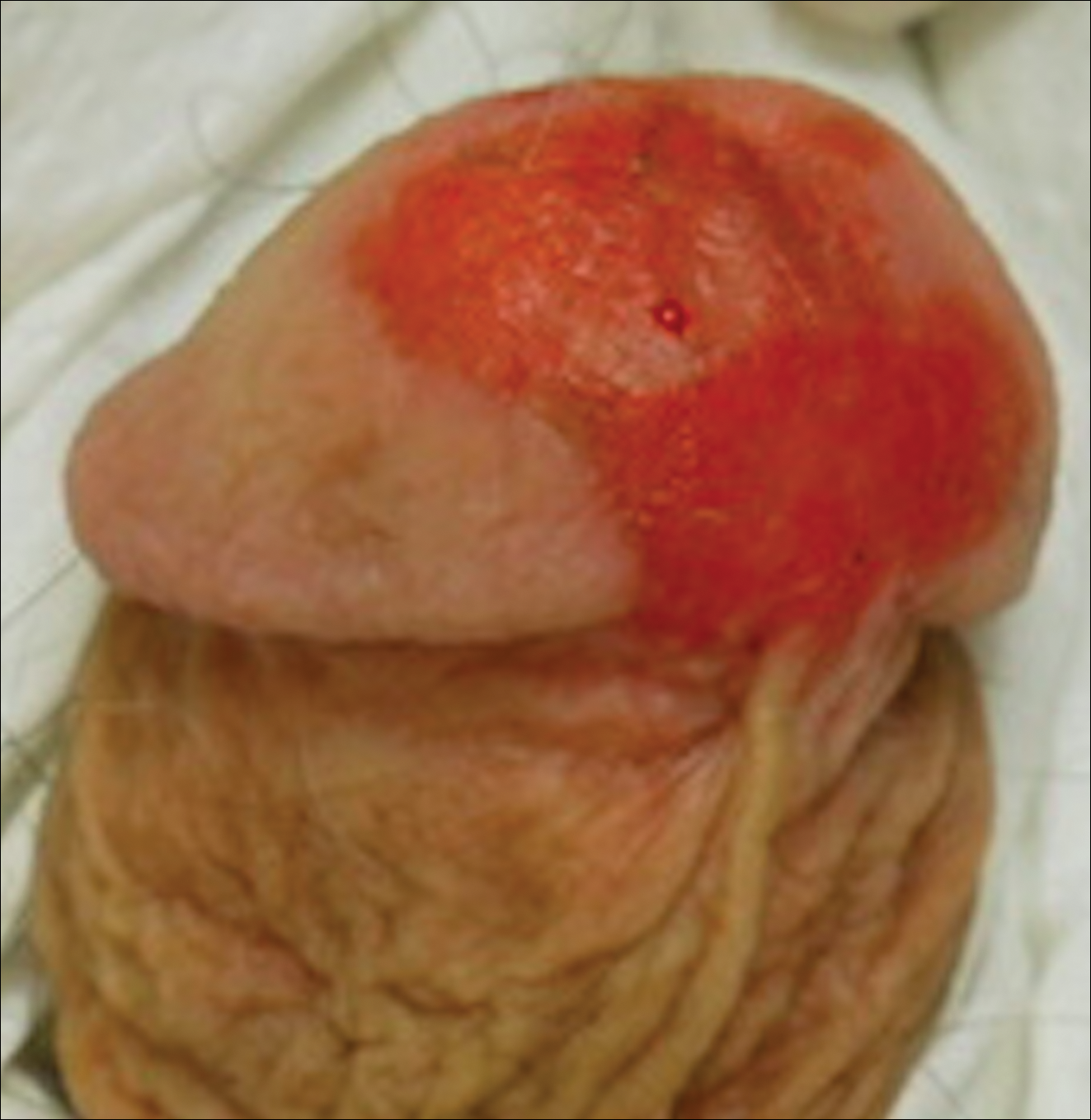
Figure 1. Penile squamous cell carcinoma. Physical examination revealed an ill-defined, 2.2 × 1.9-cm, pink, eroded plaque involving the tip of the penis and surrounding the external urinary meatus of 6 years’ duration. There was no palpable inguinal lymphadenopathy.
Distal penectomy and lymph node biopsy was recommended following evaluation by the urologic oncology department, but the patient declined these interventions and presented to our dermatology department (A.H.) for a second opinion. The tumor, including the invasive perineural portion, was removed using MMS several weeks after initially presenting to urologic oncology. Ventral meatotomy allowed access to the SCC in situ portion extending proximally up the pendulous urethra (Figure 2). Clear margins were obtained after the eighth stage of MMS, which required removal of 4 to 5 cm of the distal urethra (Figure 3). Reconstruction of the wound required urethral advancement, urethrostomy, and meatoplasty. A positive outcome was achieved with preservation of the length and shape of the penis as well as the cosmetic appearance of the glans penis (Figure 4). The patient was satisfied with the outcome. At 49 months’ follow-up, no evidence of local recurrence or disease progression was noted, and the distal urethrostomy remained intact and functional.

Figure 2. Ventral meatotomy performed in a patient with penile squamous cell carcinima requiring multiple stages of Mohs micrographic surgery allowed access to the in situ portion of the tumor extending proximally along the pendulous urethra. The fourth stage of Mohs micrographic surgery is shown here.
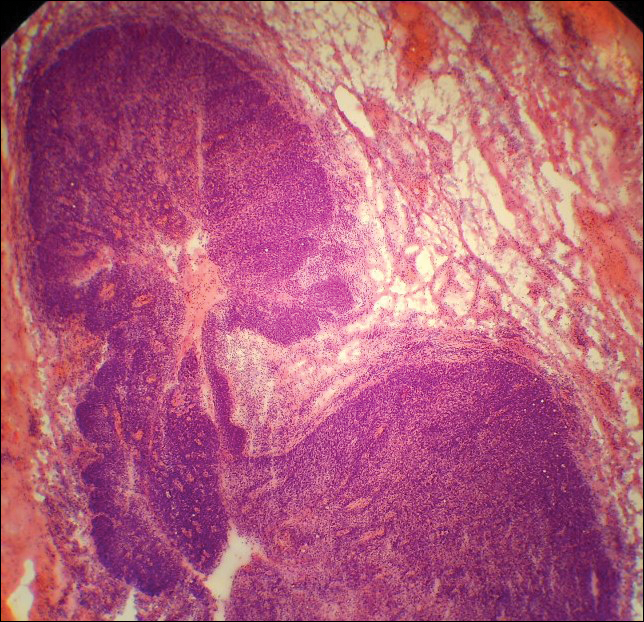
Figure 3. Low-power microscopic view of the fourth Mohs micrographic surgery stage showed squamous cell carcinima in situ with epithelial cell proliferation abutting upon the urethra (H&E, original magnification ×20).

Figure 4. Reconstruction of the wound following ventral meatotomy in a patient with penile squamous cell carcinoma required urethral advancement, urethrostomy, and meatoplasty. A positive outcome was achieved with regard to preservation of the length and shape of the penis and the appearance of the glans.