MONTEREY, Calif. — Stainless steel embedding wells may be the best of several mechanisms available to flatten or “conform” tissue specimens for sectioning in Mohs surgery, in one expert’s opinion.
Sectioning of the peripheral/epidermal margin of the lesion is essential for Mohs surgery to ensure complete margin assessment. Most Mohs surgeons require that 90% or more of the epidermis be present to feel that they’re assessing an adequate epidermal margin, Dr. David F. Butler explained at a meeting of the American Society for Mohs Surgery.
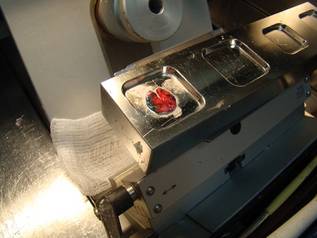 Photo courtesy Dr. David F. Butler
Photo courtesy Dr. David F. Butler
A frozen specimen is shown adhered to a stainless steel embedding well prior to application of the OCT compound.
Only two mechanisms can flatten multiple tissue specimens at once: the $20,000 CryoHist machine, or the $529 stainless steel embedding wells, said Dr. Butler, chair of dermatology at the Scott and White Hospital and Clinic and professor of medicine at Texas A&M University, both in Temple, Tex.
Lower cost, convenience, and quality results make him a fan of the stainless steel embedding wells, which consist of 1-inch steel bars with wells cut out in different sizes and depths. The bars reside within a cryostat, which provides a heat sink for the rapid freezing of the specimen.
The surgeon or other operator places a specimen facedown on the smooth surface of a well and presses down on the peripheral edge of the specimen with a gloved finger. “Like putting your tongue to a cold flagpole in Wisconsin in winter, it sticks,” he said.
Optimal cutting temperature (OCT) compound—a cryopreservation medium—is then applied over the specimen, and a metal chuck with a cross-grid pattern to better hold onto frozen OCT is applied to the OCT. A freezing block that’s been kept cold within the cryostat can be placed over the stem of the chuck to freeze the specimen more quickly.
As Dr. Butler described it, one of the sets includes one freezing bar with a 24-mm well, a 36-mm chuck, and the overchuck freezing block. He described the complete set as three bars with different well sizes, six small chucks, four large chucks, four overchuck freezing blocks, a chuck bin, an elevated embedding block, and angled freezing forceps.
The stainless steel embedding wells are available from Dr. Stephen R. Peters, the pathologist who designed them, Dr. Butler said. Dr. Peters is at Hackensack (N.J.) University Medical Center and can be reached through his Web site or via e-mail.
In using the stainless steel embedding wells for seven consecutive specimens, Dr. Butler found that five of the seven specimens (71%) met the goal of having more than 90% of the epidermis present by the sixth retained section.
He compared the time needed to freeze a specimen and mount the block using several mechanisms. It took 105 seconds with the embedding wells, 56 seconds with the CryoHist, 68 seconds with the Miami Special, and 91 seconds with the Cryocup. Only the embedding wells and CryoHist could freeze and mount multiple specimens at the same time “so the overall process doesn’t take very long,” he said.
The CryoHist is a large machine, plumbed for liquid nitrogen that flattens specimens via a vacuum suction. Compared with embedding wells, its disadvantages include the high cost and the need for greater space, external power and liquid nitrogen, and consumables such as a plastic film that is used in the process, Dr. Butler said.
The Miami Special is a long-handled clamp with flat metal plates at the end on which partially frozen OCT and a chuck are placed. The specimen is placed on the OCT and the clamp is closed and dipped in liquid nitrogen to freeze. “The problem is that it’s very cumbersome and can only do one at a time,” he said.
The Davidson Cryocup is a metal device with a long handle and a cup at one end in which tissue is placed facedown and covered with OCT and a chuck. The cup is lowered into liquid nitrogen to freeze. “It has the same problem as the Miami Special: You can only process one specimen at a time,” he said.
Other mechanisms include the inexpensive cryomold, small plastic trays of different sizes and depths on which specimens are placed facedown and covered with OCT and a chuck before placement in a cryostat. The plastic cryomold is peeled back before sectioning, one specimen at a time.
An older technique employs a heat extractor that resides within some cryostats and remains cold. A chuck is placed on the rack within the cryostat, OCT is applied, and the specimen is placed “deep side up” on the OCT, he said. A cold round bar of the heat extractor is pressed down on the specimen and OCT until frozen.