To the Editor:
Cutaneous reactions to tattoos are common and histologically diverse. As outlined by Jacob,1 these reactions can be categorized into 4 main groups: inoculative/infective, hypersensitive, neoplastic, and coincidental. A thorough history and physical examination can aid in distinguishing the type of cutaneous reaction, but diagnosis often requires histopathologic clarification. We report the case of a patient who presented with painful indurated nodules within red ink areas of new and preexisting tattoos.
A 48-year-old woman with no prior medical conditions presented with tender pruritic nodules at the site of a new tattoo and within recently retouched tattoos of 5 months’ duration. The tattoos were done at an “organic” tattoo parlor 8 months prior to presentation. Simultaneously, the patient also developed induration and pain in 2 older tattoos that had been done 10 years prior and had not been retouched.
Physical examination revealed 2 smooth and serpiginous nodules nested perfectly within the new red tattoo on the left medial ankle (Figure 1A). Examination of the retouched tattoos on the dorsum of the right foot revealed 4 discrete nodules within the red, heart-shaped areas of the tattoos (Figure 2A). Additionally, the red-inked portions of an older tattoo on the left lateral calf that were outlined in red ink also were raised and indurated (Figure 3A), and a tattoo on the right volar wrist, also in red ink, was indurated and tender to palpation. The remainder of the physical examination was normal.
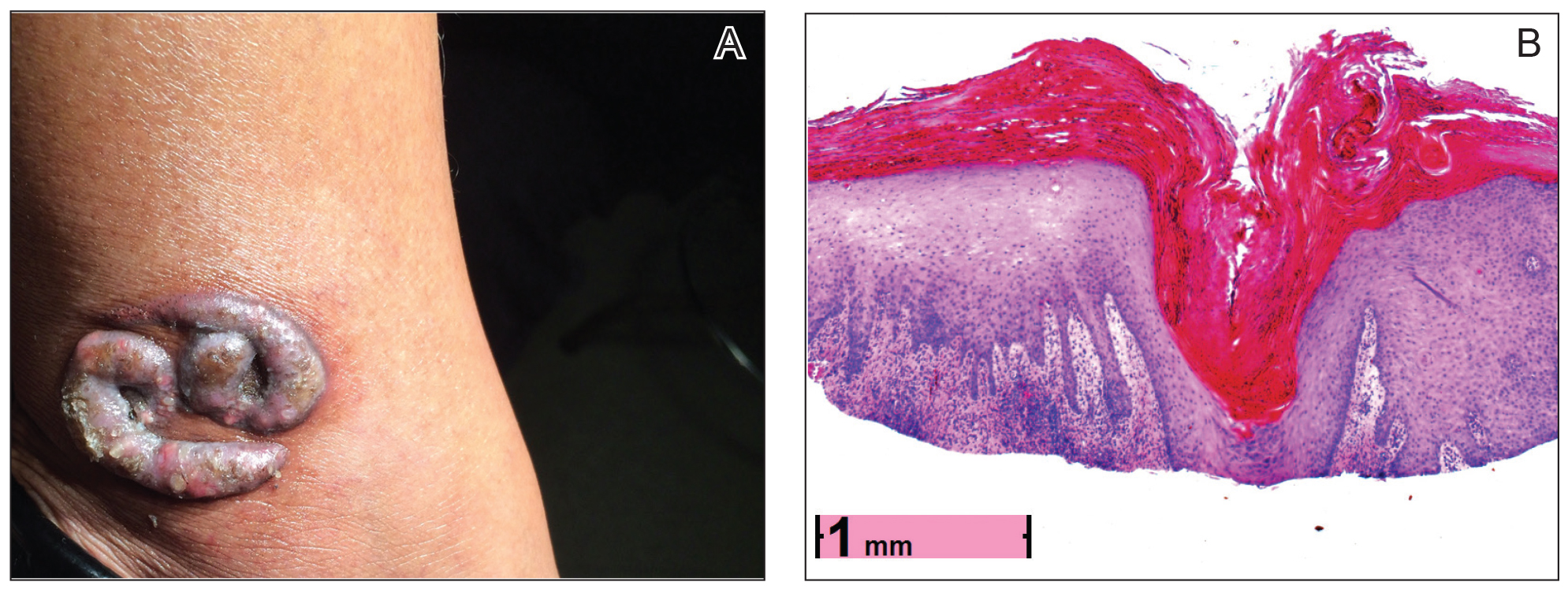
Figure 1. A, Discrete, smooth, and serpiginous nodules nested perfectly within the new red tattoo on the left medial ankle, measuring approximately 4×3 cm in diameter. B, A shave biopsy revealed crateriform neoplasm in the dermis composed of aggregates of 2 types of atypical keratinocytes, including ones with abundant eosinophilic cytoplasm and basal ones with large hyperchromatic nuclei, consistent with an early keratoacanthoma (H&E, original magnification ×2.2).
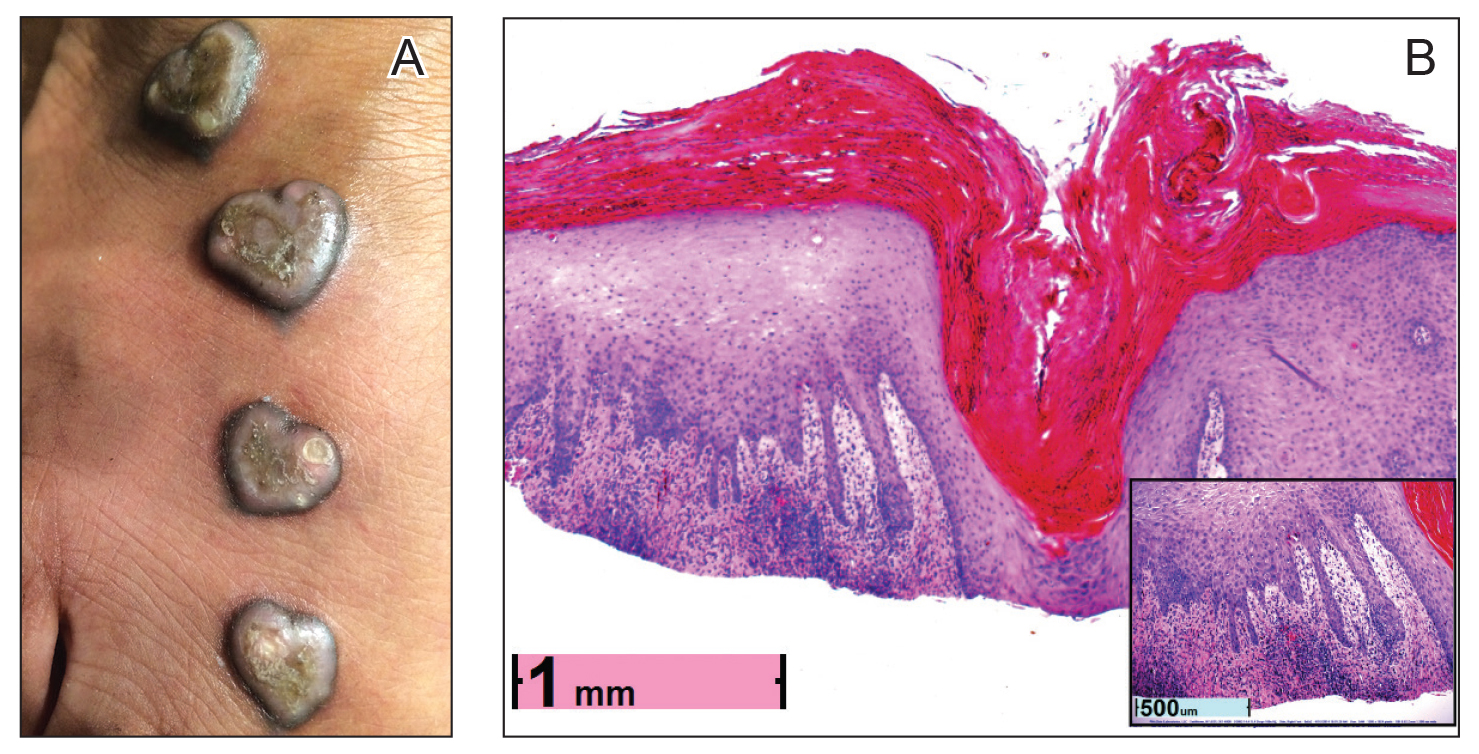
Figure 2. A, Four discrete nodules within the red, heart-shaped areas of retouched tattoos on the dorsum of the right foot, measuring 1.0 to 1.5 cm in diameter. B, A shave biopsy revealed
contiguous dilated follicular infundibula with atypical keratinocytes that had hyperchromatic nuclei, consistent with a keratoacanthoma, as well as a lymphocytic infiltrate in the dermis above a dense infiltrate of lymphocytes and histiocytes (H&E, original magnification ×2.5 [original magnification ×6.2]).

Figure 3. A, Raised and indurated borders within the red ink areas of a 10-year-old tattoo on the left lateral calf that had not been recently retouched. B, A shave biopsy revealed an infiltrate of histiocytes with granulomas (H&E, original magnification ×7.3). Multinucleated cells with granular red foreign matter were seen within some histiocytes, consistent with a granulomatous foreign body reaction (arrow)(left inset, original magnification ×86). No neoplasm was noted. Polarized light examination revealed granular refractile foreign matter in the tissue, which glowed a fluorescent coral color (arrow)(right inset, original magnification ×122).
The lesions continued to enlarge and become increasingly painful despite trials of fluticasone propionate cream 0.05%, clobetasol propionate gel 0.05%, a 7-day course of oral levofloxacin, and a 10-day course of oral amoxicillin-clavulanate. Ultimately, a shave biopsy from the new tattoo on the left medial ankle revealed an early keratoacanthoma (KA)(Figure 1B). Subsequent shave biopsies of the retouched tattoos on the dorsal foot and the preexisting tattoo on the calf revealed KAs and a granulomatous reaction, respectively (Figures 2B and 3B). The left ankle KA was treated with 2 injections of 5-fluorouracil without improvement. The patient ultimately underwent Mohs micrographic surgery of the left ankle KA and underwent total excision with skin graft.