LAS VEGAS - Practical phototherapy means not thinking strictly in terms of protocols, according to Dr. Kenneth B. Gordon.
Many protocols have been published for psoriasis phototherapy, and good ones were published by the American Academy of Dermatology in early 2010 (J. Amer. Acad. Dermatol. 2010;62:114-35), said Dr. Gordon of the University of Chicago. The guidelines emphasize tailoring therapy to meet the individual patient’s needs, and physicians should consider the best treatment for each patient.
"Simple, published protocols are not sufficient if you really do phototherapy," Dr. Gordon said.
He challenged the audience members with a quiz to test their knowledge of practical phototherapy in particular cases. The cases excluded patients with psoriatic arthritis.
"There are no right answers to these questions," Dr. Gordon said. "There are some wrong answers to these questions, however."
The Quiz Cases
– Case 1: What method of phototherapy would you use to treat a young woman with limited plaque psoriasis, primarily on her elbows? (a) Whole-body narrow-band UVB, (b) Targeted narrow-band-UVB with excimer laser, or (c) Topical psoralen plus long-wave UVA (PUVA).
– Case 2: What type of phototherapy would you use for a 50-year-old woman with extensive plaque psoriasis and type II skin who has not responded to topical therapy? She lives across the street from your office, can come for treatment in the middle of the day, and has no copay on her insurance. (a) Targeted narrow-band UVB, (b) Broad-band UVB, (c) Narrow-band UVB, (d) Retinoids plus UVB, or (e) PUVA.
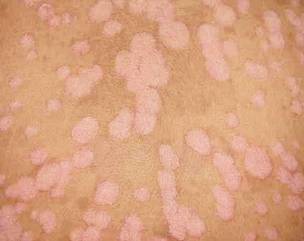 Photo courtesy Dr. Lawrence F. Eichenfield.
Photo courtesy Dr. Lawrence F. Eichenfield.
Guttate psoriasis, shown here, can be treated with narrow-band UVB with expectation for short-term treatment.
– Case 3: How would you treat an 18-year-old man having an acute outbreak of guttate psoriasis, with explosive small plaques all over the body? (a) Narrow-band UVB with expectation for short-term treatment, (b) Narrow-band UVB with expectation of long-term maintenance, (c) PUVA, or (d) Biologic immunotherapy.
– Case 4: What’s the best phototherapy for a 59-year-old woman with palmar psoriasis that is interfering with her family business, a packing company? (a) Targeted narrow-band UVB phototherapy using an excimer laser, (b) Phototherapy using a using a hand-foot narrow-band UVB unit, (c) Oral PUVA with a hand-foot UVA unit, or (d) Topical PUVA with a hand-foot UVA unit.
 Photo courtesy Dr. Gerald Krueger.
Photo courtesy Dr. Gerald Krueger.
Palmar psoriasis, shown here, can be treated with topical PUVA with a hand-foot UVA unit.
– Case 5: Which phototherapy would you choose for a 53-year-old man with extensive plaque psoriasis with big, thick plaques, including many on his back? (a) Targeted UVB with excimer laser, (b) Narrow-band UVB, (c) Retinoids plus narrow-band UVB, or (d) PUVA.
– Case 6: How would you treat a 52-year-old man with type I skin who has had plaque psoriasis for years but has become erythrodermic over the past 6 months? (a) Narrow-band UVB, (b) Retinoids plus UVB, (c) PUVA, (d) Targeted phototherapy with excimer laser, or (e) None of the above.
Answers
– Case 1: Dr. Gordon said he would choose (b) Targeted narrow-band UVB with excimer laser, although topical PUVA may be the solution sometimes, he added.
Targeted narrow-band UVB with excimer laser is "not so easy," he cautioned. On the plus side, two or three treatments per week for 6-12 weeks have a high chance of success, with more than 75% of patients achieving a Psoriasis Area and Severity Index (PASI) score of 75, or even better if you treat with higher-than-usual fluences. This method only treats involved areas and avoids treating normal skin. Perhaps more than half of patients will have long-term clearing of those limited areas at 1 year after treatment.
On the down side, severe and permanent hyperpigmentation is always a risk with the excimer laser, particularly when higher fluences are used, so it’s important to discuss this with patients when considering targeted UVB therapy. There also may be temporary blistering and pain.
"Application to extensive body surface areas is, in a scientific word, silly," Dr. Gordon said. "I bring that up because I have people in our community who are using it for people who have 20%-30% body surface area involved in psoriasis." In those cases, it’s better to refer the patient for other therapy or consider alternatives such as topical treatments or intralesional injections.
– Case 2: Broad-band UVB may be effective for this patient, though not as effective as narrow-band UVB. Retinoids plus UVB is a reasonable option in a postmenopausal 50-year-old woman. He does not use PUVA therapy "because of biases that I developed during my residency," he said.