Calcipotriene–Betamethasone Dipropionate Topical Suspension in the Management of Psoriasis: A Status Report on Available Data With an Overview of Practical Clinical Application
From the Touro University College of Osteopathic Medicine, Henderson, Nevada, and Las Vegas Skin and Cancer Clinics/West Dermatology Group, Las Vegas and Henderson.
Dr. Del Rosso is an advisory board member, consultant, and speaker for Allergan, Inc; Bayer Health Care Pharmaceuticals; Galderma Laboratories, LP; LEO Pharma; Promius Pharma; PuraCap Pharmaceutical; Ranbaxy Laboratories Limited; Taro Pharmaceuticals USA, Inc; and Valeant Pharmaceuticals International, Inc. He also is a consultant for Aqua Pharmaceuticals, and is a researcher for Allergan, Inc; Bayer Health Care Pharmaceuticals; Galderma Laboratories, LP; LEO Pharma; and Valeant Pharmaceuticals International, Inc.
Psoriasis is a multifactorial process associated with immunologic dysregulation. Chronic plaque psoriasis (PP) is the most common clinical presentation. Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of topical corticosteroid (TC) therapy along with concurrent or sequential use of a nonsteroidal topical agent is commonly employed to achieve and sustain control of the disorder. Calcipotriene 0.005%–betamethasone dipropionate 0.064% topical suspension (C/Bd-TS) is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP. This article provides a review of a patented topical suspension combination formulation of C/Bd-TS, including formulation characteristics, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies.
Calcipotriene 0.005%–betamethasone dipropionate 0.064% topical suspension (C/Bd-TS) applied once daily has been shown in multiple studies to be effective, well tolerated, and safe for the treatment of plaque psoriasis (PP) involving the scalp and/or other body sites such as the trunk and extremities. Studies have included all severities of PP, with both investigator and subject assessments shown to be favorable overall.
Most studies were completed in adults over a duration of 8 weeks; however, clinical trials also have been performed with C/Bd-TS in adults treated for up to 52 weeks for scalp psoriasis, in a subgroup of Hispanic/Latino and black/African American adult patients with scalp psoriasis, and in adolescents with scalp psoriasis.
Studies evaluating application of C/Bd-TS once daily for PP affecting nonscalp sites have primarily involved use on the trunk and extremities.
The adaptability for scalp and body application allows for use in many cases of a single topical product without needing to prescribe a second leave-on medication specifically for use on the scalp.
References
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
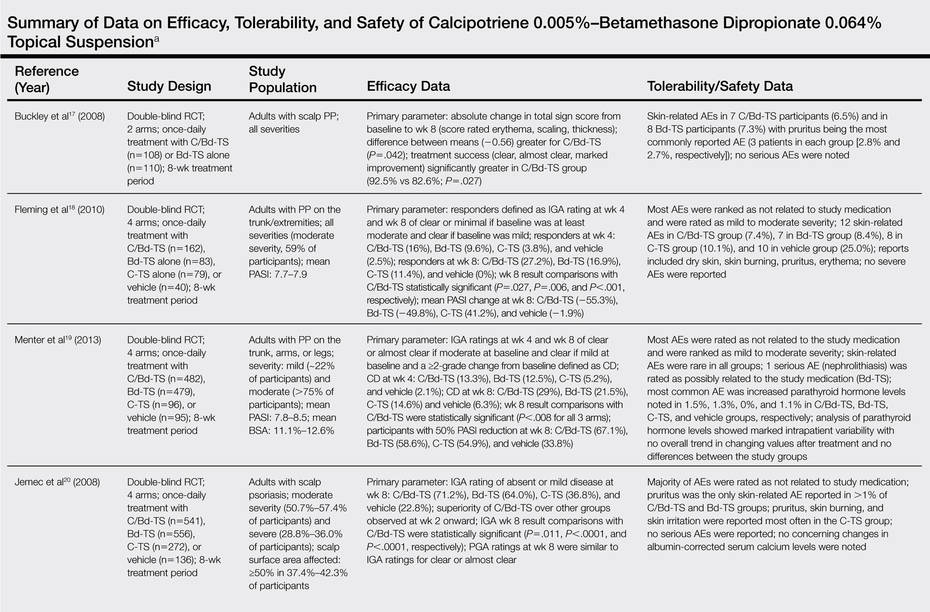
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.