SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
Dr. James T. Rosenbaum
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
 Copyright 2015 ACR
Copyright 2015 ACR
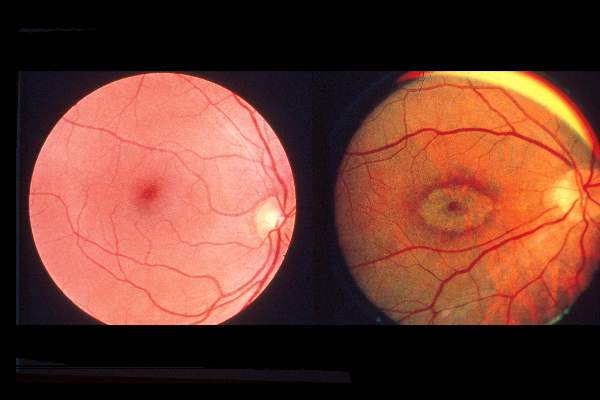
Fundoscopic images show early and late “bulls-eye” lesions.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.