Kelsey Rife, Alessandra Lyman, and Kristina Pascuzzi are Clinical Pharmacy Specialists; Corinna Falck-Ytter is the Section Chief of Primary Care, Christopher J. Burant is a Statistician in the Geriatric Research, Education, and Clinical Center; and Yngve Falck-Ytter is the Section Chief of Gastroenterology and Hepatology; all at the VA Northeast Ohio Healthcare System in Cleveland. Sheena LeClerc-Kamieniecki is a Clinical Pharmacy Specialist at the Chillicothe Veterans Affairs Medical Center in Ohio. Corinna Falck-Ytter is an Associate Professor of Medicine, Christopher Burant is an Associate Professor of Nursing, and Yngve Falck-Ytter is a Professor of Medicine, all at Case Western Reserve University in Cleveland, Ohio. Correspondence: Kelsey Rife (kelsey.rife@ va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The primary endpoint was the change in HbA1c up to 4 months posttreatment in patients achieving SVR12. Secondary endpoints included the sustained change in HbA1c up to 12- and 18-months posttreatment, as well as change in antihyperglycemic medications from baseline to the end of HCV treatment and from baseline to 3 months posttreatment in patients achieving SVR12. Lastly, the changes in HbA1c and net changes in antihyperglycemic medications were compared among patients who achieved SVR12 and those who relapsed.
Statistical Analysis
The anticipated sample size after inclusion and exclusion for this study was 160 patients. As HbA1c is a continuous variable and tested prior to treatment and up to 18-months posttreatment, a paired dependent 2-sided t test was used for this study. For a paired dependent t test with an α of 0.05 and a power of 80%, a sample size of 160 would be able to detect a moderately small, but clinically relevant effect size of 0.22. Descriptive statistics were used for secondary outcomes. For categorical data, frequencies and percentages are provided.
Results
A total of 437 patients were identified as having a diagnosis of T2DM and being prescribed a HCV DAA, of which 157 patients met inclusion criteria. The 280 excluded patients included 127 who were not on antihyperglycemics at the start of HCV treatment, 147 who did not have HbA1c data within the specified time frame, 4 were excluded due to delayed treatment initiation outside of the study time period, and 2 self-discontinued HCV treatment due to adverse drug reactions.
Baseline Demographics
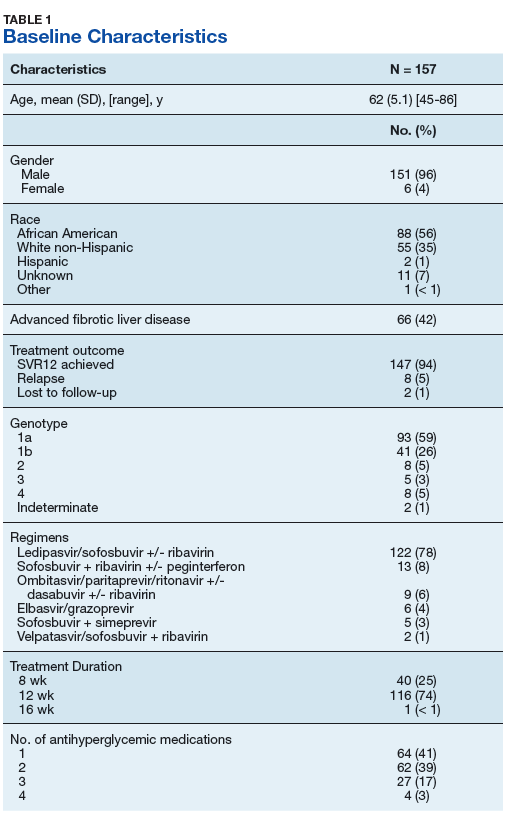
The majority of patients were male (96%), primarily African American (56%), with a mean age of 62 years (Table 1).
Nearly half of the patients were deemed to have advanced fibrotic liver disease, and most had genotype 1 HCV (85%). The majority of patients were taking ledipasvir/sofosbuvir +/- ribavirin (78%) and achieved SVR12 (94%), while 59% were treated with ribavirin. Of the 10 patients who did not achieve SVR, none were treated with a second HCV regimen during the study period. Most patients were either on a monotherapy (41%) or dual (39%) therapy antihyperglycemic regimen.
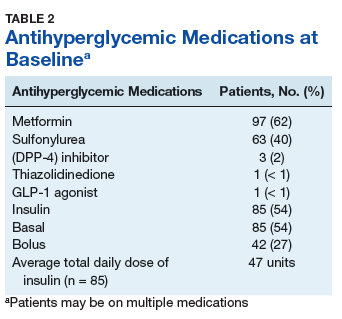
Metformin was the most commonly prescribed antihyperglycemic medication (62%), followed by insulin (54%), and sulfonylureas (40%) (Table 2).
No patients were on sodium-glucose cotransported-2 (SGLT-2) inhibitors as these were still new to the market during the study’s time frame. The mean total daily dose of insulin was 47 units at baseline. Half of all included patients were on basal insulin, and 27% of patients were on a basal/bolus insulin regimen.
Primary and Secondary Endpoints
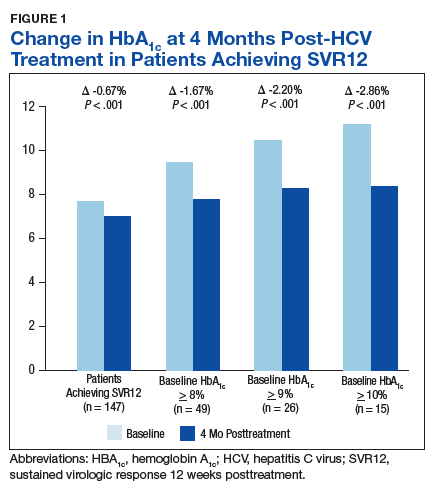
There was a significant immediate HbA1c lowering of 0.67% (from 7.67% to 7.00%; P < .001) in patients who achieved SVR12 over a mean of 2-months posttreatment (Figure 1).
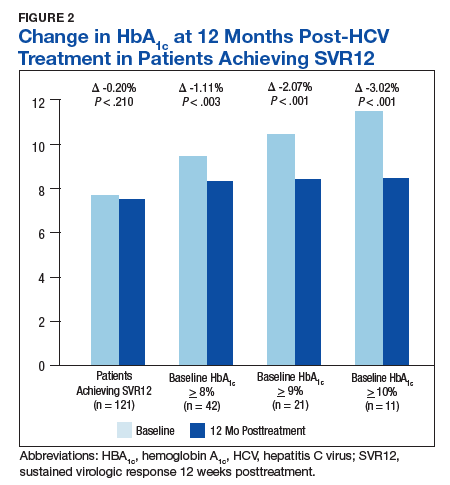
Patients who achieved SVR12 (121 of 147) had follow-up HbA1c data up to 12 months posttreatment, for which the overall HbA1c lowering was 0.20% (P = 0.21) (Figure 2).
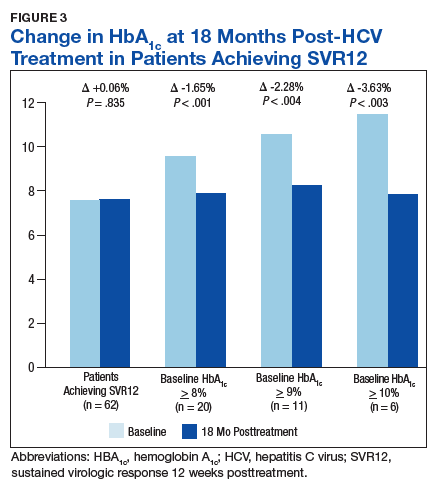
In the overall cohort of patients achieving SVR12, the HbA1c lowering was not sustained at 18 months posttreatment. However, a subanalysis demonstrated that patients with baseline HbA1c ≥ 8%, ≥ 9%, and ≥ 10% had an increasingly larger HbA1c Δ upon HCV treatment completion; the change in HbA1c for these subcohorts did remain significant at sustained time points. Patients with a baseline HbA1c ≥ 8%, ≥ 9%, and ≥ 10%, showed 18-month posttreatment HbA1c decreases of 1.65% (P < .001), 2.28% (P = .004), and 3.63% (P = .003), respectively (Figure 3).
By the end of HCV treatment, 20% of the patients who achieved SVR12 had a de-escalation of their antihyperglycemics. This increased to 30% by 3 months posttreatment among those achieving SVR12, in contrast to 13% of patients in the relapse group (Figure 4).
Of the 8 patients who relapsed, there was a significant decrease in HbA1c of 0.90% from 7.54% to 6.64% (P = .024) at 4 months posttreatment. Of the relapsers who had HbA1c values up to 12 months and 18-months posttreatment, the observed change in HbA1c was 0.61% and 0.2%, respectively. However, the data are limited by its small numbers. One (13%) of the HCV treatment relapsers had an escalation of their antihyperglycemic regimen, while 1 (13%) had a de-escalation, and the remaining 6 (75%) had no change.