DR. IZZO: I am honored to moderate today’s discussion with 3 very well recognized experts in hypertension: true “doctor’s doctors,” if you will. Our panelists include Dr. Jan Basile from South Carolina, Dr. Alan Gradman from Pittsburgh, and Dr. Marvin Moser from New York. Welcome, gentlemen.
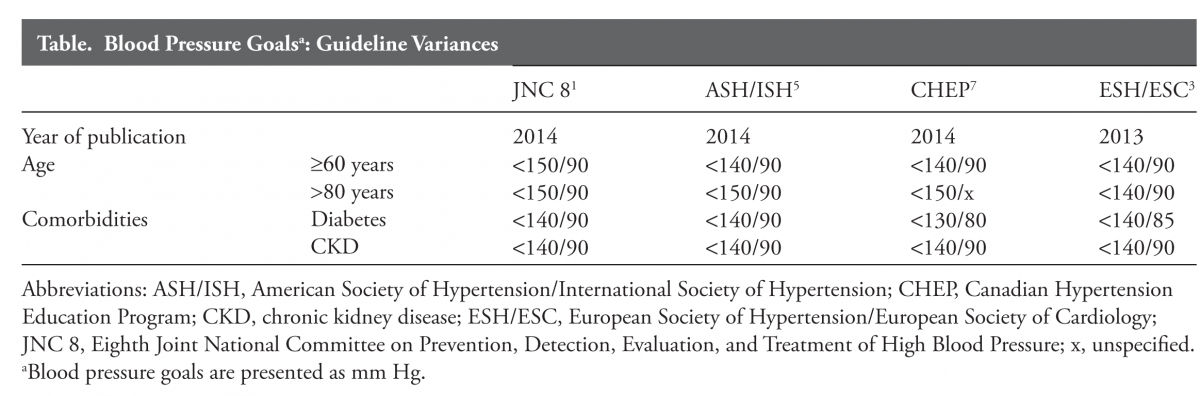
The first part of our discussion focuses on the issue of guidelines and guideline proliferation. Over the last several years, multiple professional groups and health-associated agencies have issued guidelines for the diagnosis and treatment of hypertension. It is not clear to me that these competing documents provide a rational platform for improved care. Despite some recent claims, no guideline can be fully “evidence-based” because we cannot afford clinical trials for each relevant clinical question. Furthermore, the current batch of new guidelines has yielded conflicting recommendations. For example, the definition of “elderly” as age 60 in the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) and age 80 in the recent joint guidance from the International and American Societies of Hypertension. I fear that the guideline process has essentially broken down—this benefits no one.
First, a little history. Prior JNC documents were produced under the auspices of the National High Blood Pressure Education Program, a consortium of about 3 dozen healthcare professional organizations. As a participant in JNC VI and JNC 7, I can assure you that all participants were dedicated scientists and clinicians whose common goal was to synthesize the best and most robust information into a document that provided practitioners with the most reliable guidance possible. JNC 7 was released in 2003 and was soon widely adopted; it truly stood the test of time. After that, everything changed. Dr. Basile, what has been happening since?
DR. BASILE: Thanks, Dr. Izzo. I agree with you about your concerns with guidelines. This is a very difficult issue for the practicing clinician.
With regard to JNC 8, in 2008, the National Heart, Lung, and Blood Institute (NHLBI) decided to develop its own comprehensive “evidence-based” disease prevention portfolio that included a coordinated cholesterol guideline, obesity guideline, hypertension guideline, as well as a lifestyle/risk factor modification guideline. Following the recommendations put forth by the Institute of Medicine on guidelines, the NHLBI mandated that strict rules of evidence be used for its guideline development. After the JNC 8 committee established the clinical trial criteria for use in their hypertension guideline, the NHLBI hired a professional vendor to vet the literature. The process was essentially going nowhere so a second vendor for hypertension had to be hired. In the end, few clinical trials passed the criteria used to form the basis of JNC 8. And near its completion, after the JNC 8 group toiled for over 5 years putting their report together, they learned in 2013 that the NHLBI withdrew its support for the guideline and asked the American College of Cardiology/American Heart Association to establish a joint task force (to include the JNC 8 group) to assume responsibility for the guideline process. Declining this collaborative opportunity, the JNC 8 group decided on their own to have their work submitted and it was published without organizational support in JAMA.1
Meanwhile, the Centers for Disease Control published an overall systems approach for primary care clinicians in which they released the Kaiser Permanente algorithm for effective blood pressure (BP) control.2
Of note, there are several other competing guidelines: one which is issued annually by the Canadian Hypertension Education Program. This approach is now extremely well developed and comprehensive with multiple web-based programs and information sources (www.hypertension.ca/en/chep). In addition, there is the recent effort by the European Society of Hypertension/European Society of Cardiology in 2013,3 and a newer, less formal document from the International Society of Hypertension and supported by a working group comprised of members of the American Society of Hypertension.4 Finally, there are other national guidelines around the world, perhaps most prominent among these being the British Hypertension Society National Institute for Clinical Excellence or the NICE guidelines.
DR. IZZO: That’s a good summary, Dr. Basile. What constitutes a useful guideline? Who is the audience? I don’t believe that a good guideline should be hidebound by unduly restrictive ‘evidence rules’ that ignore all but a tiny fraction of the available scientific information. A good guideline must synthesize complex data in a clear and concise way and must address the kinds of questions that real doctors need answered every day. Dr. Gradman, do you have an opinion on guidelines?
DR. GRADMAN: Part of what is going on in the revised hypertension guidelines is a worldwide shift from the treatment of individual patients to the treatment of patient populations. Such guidance for treating large groups is of great interest to governments and insurance companies but is less useful for making treatment decisions for individual patients with individual problems.
In fact, the JNC 8 guidelines specifically say that they are aimed at primary care physicians, not specialists or people who have a lot of experience with the treatment of hypertension. I think JNC 8 is to be commended for trying to make the fundamental concepts of the guidelines completely evidence-based. The guidelines delineate general targets and thresholds for treatment and also suggest the best drugs to use for most patients. Unfortunately, the exercise showed that it is not really possible to answer a lot of specific treatment questions using a strict evidence-based approach. For these we must rely on less definitive evidence and expert opinion.
I think there are different audiences; a good general guideline today should be aimed at primary care physicians but I think specialists need their own guidelines. As a cardiologist, I would want a very different set of guidelines than is presented in JNC 8.
DR. IZZO: Dr. Moser, given your long association with the highly successful parent of the JNC process, the National High Blood Pressure Education Program, I think your perspective is invaluable. Do you think any of the current guidelines hit the mark or what do you think should have been done differently?
DR. MOSER: Well, that’s a broad question. JNC 8 doesn’t differ much from JNC 7 except for one or 2 items. JNC 8 set out to answer several questions with a strict evidence-based methodology, and when they were finished, after a long period of time and substantial expenditure of money, they only ended up addressing 3 questions. The first question was when to initiate treatment, the second was related to the target or goal BPs, and the third was how to achieve goal pressures. They did address the question of whether people with comorbidities, especially diabetes and kidney disease, needed to have lower goal BPs.
On the issue of targets for BP, it was decided that 140/90 mm Hg was good enough for most people and that there was no compelling evidence that BP should be lowered below 130/80 mm Hg in diabetics or people with kidney disease. But we all know that in practice, you can’t adjust BPs to exact numbers. JNC 8 also said that the threshold for a diagnosis and target BP in people over the age of 60 was 150/90 mm Hg. This is quite different from other guidelines.
The guidelines also point out a difference in black and white patients. We’ve known for years that calcium-channel blockers (CCBs) and thiazide-type diuretics are more effective in blacks and angiotensin-converting enzyme (ACE) inhibitors or beta blockers are more effective in whites, so I don’t think JNC 8 provided any new information on this. Otherwise, you’ll find very little difference between JNC 8 and 7. What they didn’t address were possible changes in the diagnostic evaluation or nonpharmacologic therapy and they failed to discuss issues related to the delivery of care and adherence, etc. Some physicians have said that the changes are important and different, but when you look at it very carefully they’re not substantive compared to other reports.
Dr. IZZO: Is that a result of their strict rules of evidence?
Dr. MOSER: The report was supposed to be all evidence-based. They hired an outside vendor that reviewed about 6100 English-language papers. The experts on that panel could have picked up the 40 papers that they finally rated as acceptable within a few days. It took the vendors several years. As everyone has mentioned, they used the data from evidence-based trials and reached conclusions, but they also had an “out” on all of them, including the 150 mm Hg BP target in the elderly, which was arbitrarily defined as age 60. As in their other recommendations, they then said that you could rely on “expert opinion,” meaning clinical judgment. This is the basis of the major recommendation: “If you treat below 140/90 mm Hg and everybody’s happy and there are no side effects, then just continue treatment.”
Regarding their approach to the treatment of resistant patients, the proposed algorithm is almost the same as it has been for many, many years. So I’m very disappointed in what they have accomplished, especially since it took such a long period of time and cost so much money.
DR. IZZO: I echo your disappointment, especially on very fundamental grounds. First, a guideline constrained by the suffocating rules applied by the JNC 8 group is enormously biased, especially when over 99% of the potentially relevant information was ignored because it did not come from a randomized trial. Did they not understand just how biased randomized clinical trials really are? A true expert does better than that, prioritizing the value and relevance of all evidence, from bench science to randomized trials. The real test for a guideline is then in the projection of that synthesis, that is translating expert interpretation into understandable and workable recommendations. One other issue: absence of evidence should not imply a negative recommendation. If there is no definitive study proving that a lower BP target is warranted for people with kidney disease, it should also be very clear that there is existing evidence that lowering BP to 130/80 mm Hg instead of 140/90 mm Hg may be a good idea. JNC 8 chose to ignore studies of achieved (not intention-to-treat) BP values that identified better renal outcomes in diabetics5 and fewer recurrent strokes6 in trial participants with the lowest BPs. While it is true that such benefits are not achieved by all trial participants, it should be recognized that “lower is better” is probably true in at least some people.
Are there any comments or concerns that the narrow definition of evidence can actually lead us astray?
DR. BASILE: I appreciate your points, Dr. Izzo, they’re very important for the clinician. Regarding guidelines overall, I like Dr. Gradman’s points about the individualization versus the population strategy. The one-size-fits-all guidelines just do not apply to the many heterogeneous patients we see.
The JNC 8 tried to be an evidence-based document in that they only looked at randomized controlled hypertension trials, which in itself is a limitation. These were very strict criteria that prevented the group from including certain evidence bases. But ultimately, more than half of the guideline recommendations ended up being expert opinion. And the reason they ended up addressing only the 3 questions presented is because there just isn’t the kind of clinical trial-based evidence required to answer questions on issues such as resistant hypertension, the value of combination therapy, and contrasting differences in BP measurement techniques to detect which is best. Accordingly, we end up with a somewhat narrow perspective. In fact, JNC 8 ended up with a lot of expert opinion and failed to be as evidence-based as they would’ve liked to have been. At the end of the day, JNC 8 just doesn’t provide the clinician with the answers to many of the controversial issues that we face each and every day.
DR. IZZO: I’m with you on that last point, Dr. Basile. Speaking of evidence, although we know that systolic BP rises linearly with age, where is the study justifying that after age 60, your BP threshold should be relaxed immediately? JNC 8 said there is “no evidence of a BP benefit here”; I say there is no evidence of common sense here.
DR. BASILE: The recent American Society of Hypertension/International Society of Hypertension (ASH/ISH) guideline suggests that “elderly” means 80 years of age and older. The JNC 8 panel decided that while some trials had higher thresholds for eligibility than the BP goals tested, in an effort to simplify the message they decided that the threshold for initiating antihypertensive treatment should be made the same as the BP treatment goal. So their answer to the second question, “What should be the goal for BP reduction in patients who are 60 years of age and older?” is that it should be less than 150/90 mm Hg, the same as the threshold for starting antihypertensive therapy.
DR. MOSER: Well, the evidence doesn’t actually support this. None of the BP cutoffs were ever truly “evidence-based,” but the new guidelines do not acknowledge this. Clearly, evidence from randomized trials of any therapeutic benefit from having a systolic BP under 150 mm Hg isn’t very good, but expert opinion, clinical judgment, and epidemiologic data suggest very strongly to me that we should have kept the threshold for diagnosis and treatment at 140/90 mm Hg at any age. If a systolic pressure under 140 mm Hg is achieved in the elderly and therapy is well-tolerated, then therapy should be continued as before.
DR. GRADMAN: The targets for patients with diabetes and renal disease have been changed and that must be discussed. The revised goal of <140/90 mm Hg for diabetics was based primarily on the results of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial which compared that goal to a goal of <120/80 mm Hg and found no net advantage of very aggressive treatment. The JNC 7 goal of <130/80 mm Hg was never evaluated. It is of interest that the newest Canadian guidelines retain the <130/80 mm Hg recommendation.7 The JNC 8 document ignored individual patient differences, which might influence treatment decisions. In patients at increased risk for stroke, such as Asian populations or patients who have a history of cerebrovascular events, lower targets may be a rational treatment decision. As ACCORD demonstrated once again, stroke risk is exquisitely BP sensitive and those in the 120/80 mm Hg target group had fewer strokes; this consideration may trump others in specific patients. The JNC 8 document was certainly not for experts or specialists in the treatment of hypertension. Guidelines are also needed to address the “hard-to-treat patient” who may be defined in a number of ways.
DR. MOSER: Well, let me just embellish that, Dr. Izzo, for a second. If you ask who is going to use this document as a metric, or who is going to hold clinicians to these recommendations, at the end of the day, it may be no one. This is because JNC 8 was, unfortunately, not endorsed by any major group; it is a standalone document. It was sent out to a number of hypertension specialists who had an opportunity to give comments, but it wasn’t posted for either the professional community or the public community to see if there were any concerns before it was published.
I don’t necessarily mean this as a harsh criticism because it seems the JNC group was forced to go it alone. But there’s a possibility that not all major organizations, including the government, may actually accept the recommendations, especially the one relating to age and target BPs.
DR. GRADMAN: I wouldn’t agree with that entirely. I think people will latch onto the JNC document, in particular to the idea that patients don’t need to be treated as intensively as was recommended in the past. So these guidelines will reduce the number of people who are seen to require treatment and will lower the intensity of treatment for those who are receiving therapy. Computerized medical records will soon be almost universal and it will be easily determined if the practitioner is in compliance with a cutoff of 140/90 mm Hg in general or less than 150 mm Hg if a patient is over 60. So I think it could have more effect than you seem to think, Dr. Moser. Many people will conclude that lower really isn’t better. The cost of treatment to insurance companies and managed care organizations will go down as a lower intensity of treatment becomes the standard of care.
DR. BASILE: I agree with you, Dr. Gradman. The ASH/ISH and European Society documents have also abandoned the <130/80 mm Hg threshold for diabetic and chronic kidney disease (CKD) patients, in favor of a goal of <140/90 mm Hg (European Society <140/85 mm Hg in diabetes [Table]), so there is additional weight behind the new metrics in addition to JNC 8.
DR. MOSER: In response to Dr. Gradman, when you increase the target for treatment to 150 mm Hg you eliminate an enormous number of people in the “difficult-to-treat” category. Another point, some of the new guidelines are not user-friendly as Dr. Izzo pointed out. They may not be helpful for the practicing doctor. The European guidelines, for example, are too long and have too many references. I believe that JNC 8 should have been 6 or 7 pages. Physicians do not care about an A-rating, B-rating, or C-rating; they want to know what experts believe.
DR. IZZO: The European guidelines are unnecessarily complex and have other flaws, such as conflating hypertension treatment with risk scores. Interpretation and perspective are the jobs of an expert panel and those traits, labeled for what they are, need to be integral to the framework of any good guideline. That’s what JNC 7 had in greater measure and that’s what people want.
DR. IZZO: Maybe we can slightly reframe this same discussion in light of another vexing problem that seems to continue to surface. Is there a J-curve? Are there different J-curves for different organs or diseases?
DR. MOSER: The issue of J-curves has never been covered effectively.
DR. BASILE: It’s not discussed in most of the guidelines because it’s a very controversial area. In principle, there is a J-curve because when you get to a BP of 0 mm Hg, you can’t sustain life. I don’t have a problem with the JNC group or other groups not really looking into this J-curve issue but it’s a terrible problem for the clinician, never knowing what level you might put the patient in danger as you continue to lower BP.
DR. GRADMAN: I agree with you, Dr. Basile. I think the possibility that the J-curve is real underlies the changes the new guidelines made in target BPs. Higher BP targets will promote less aggressive BP-lowering, so maybe the J-curve “risk” will be diminished somewhat. Different endpoints appear to have different J-curves. You may reduce strokes, for example, but increase myocardial infarctions, and the latter seems to be related more to low diastolic BP. This risk-benefit balance of intensive treatment really underlies a lot of the changes that we’ve seen in target BPs in many guidelines, not just JNC 8. Overall attention to this equation is positive but guidance to clinicians faced with patients with specific risk factors, co morbidities, circadian BP patterns, or other clinical characteristics is completely lacking.
DR. BASILE: I totally agree with you, Dr. Gradman. Increasing the systolic BP goals will also lead to some increases in diastolic BP and perhaps less concern about J-curves, if they really exist.
One important point that I’ve been making with clinical groups is that the “ideal” BP for most patients depends on whether that patient is most at risk for stroke, heart attack, or kidney disease. These differing target organs do not all prefer to see the same amount of BP reduction. For example, the brain seems to prefer a lower target and does better with more systolic BP reduction than does the heart. Yet our antihypertensive agents are not organ specific when we use them so we have to accept a “sweet spot” that is most beneficial to the patient and causes little harm. Accordingly, I think there is a “best” BP range for most patients; the European guidelines suggest that when you keep the systolic BP for most patients between 130 and 139 mm Hg, you’re really doing the best for the patient. I agree with this. I believe this should be our “sweet spot” for most patients with hypertension except for the oldest of the old, especially those with isolated systolic hypertension, where the spot appears to be 140–149 mm Hg.
DR. IZZO: Another point worth making about risk reduction is related to the geometric nature of risk and risk reduction and the “20/10 rule.”8 At a systolic BP of 170 mm Hg, the overall cardiovascular disease risk is about 4x greater than a systolic of 130 mm Hg. Reducing the systolic from 170 to 150 mm Hg has the potential to reduce the relative risk by 50% (to 2x); going from 150 to 130 mm Hg lowers the risk to 1x overall, a 75% risk reduction from the 170 mm Hg baseline in this example. In this sense, the main benefit is getting the person out of the higher risk category, Stage 2 hypertension. The first few millimeters of mercury are the most important. Maybe this justifies the higher targets a little bit too but it’s hard to argue against the principle of “lower is better.”

DR. MOSER: We have discussed treatment targets and it appears that we disagree generally with the change from 140 to 150 mm Hg as a target in the elderly. We seem to have decided that the target BP of 140/90 mm Hg is reasonable, and perhaps the change in targets in treating the diabetic might also be reasonable, although if you could get to 130/80 mm Hg, that’s fine. I agree with Dr. Izzo, the lower the better.
I think now we probably ought to address how to get there. If you look at the JNC 8 protocol of both the treatment of lower and the high-risk patient, it’s almost exactly the same as in JNC 7. The proposed algorithm for treatment does not contribute much that is new to the clinician’s ability to treat this disease effectively. Perhaps that is because specific therapy has not changed much in the past 5–8 years. We may have learned more about how to use certain therapies, but the actual medications haven’t changed much: the specific medications recommended are almost exactly the same as in JNC 7, except for the addition of chlorthalidone and indapamide.
DR. IZZO: Well, there is one difference: thiazide-type diuretics, dihydropyridines, and ACE inhibitors (or ARBs) are now referred to as “preferred drugs,” as was first suggested in our New York State Medicaid hypertension guideline in 2011.9 We defined a preferred agent as one with appropriate efficacy and safety that is also proven to lower cardiovascular event rates. I’d be interested in the opinions of this group with regard to treatment issues and also to the specific issue of whether beta blockers were unduly excluded.
DR. BASILE: I salute JNC 8 in leveling the playing field when they suggest that it is the amount of BP reduction achieved that is more important than the initial drug, but when you look at the outcome evidence from clinical trials for stroke as well as cardiac and renal disease, you can feel very comfortable using a renin-angiotensin system (RAS)-blocking drug, either an ACE inhibitor or an angiotensin receptor blocker (ARB), or a thiazide-type diuretic or a CCB.
I’m somewhat concerned that they lumped all CCBs together because I do think there’s more evidence of benefit for the dihydropyridines or the “pines” in hypertension than the other subclasses (diltiazem and verapamil). But I like the fact that 4 major classes are now looked at as being equal for initial therapy, even in diabetics, unless they have CKD. Unless they have CKD, JNC 8 very appropriately recommends that it’s BP reduction rather than the RAS blockade that translates into improvement in outcomes. However, for the diabetic with CKD, we would recommend an ACE or an ARB as a first drug. As for the beta blockers, they do not have the level of evidence that the thiazides have had, as most trials used once-a-day atenolol as their beta blocker. We just don’t know how some of the newer beta blockers would have stacked up to the other antihypertensive agents on clinical outcomes for those with hypertension without concomitant issues.
DR. IZZO: Dr. Gradman, as a card-carrying cardiologist, wouldn’t you be thrown out of your business if you failed to advocate for beta blockers?
DR. GRADMAN: To some extent that’s true, but the guidelines that we’re talking about are a broad-brush approach. JNC 8, based its opinion regarding the first-line use of beta blockers on one study: the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial,10 which found a lower relative risk of stroke with losartan compared to atenolol. For cardiologists, beta blockers remain an essential component of treatment in the majority of patients with coronary disease, angina pectoris, and heart failure, with or without hypertension, and in patients with arrhythmias, such as atrial fibrillation. In the case of post myocardial infarction, though, it is unclear if the benefit persists, especially after 2 years.
Another criticism I have of the guidelines is that they lump all drugs from each class together. That’s especially problematic for CCBs and for beta blockers. There’s still some discussion about the variable effects of different beta blockers on glucose tolerance, side effect profile, vascular tone, and other properties.
Age may matter too, in the decision to use beta blockers. In a Canadian meta-analysis, patients under the age of 60 taking beta blockers did just as well as those taking other drugs, but beta blockers were not as effective in older patients in terms of endpoint reduction.11
In uncomplicated hypertension, though, I do agree with the broad-brush recommendations for primary care physicians that the other 4 classes of drugs (thiazide-type diuretics, ACE inhibitors, ARBs and dihydropyridine CCBs) still have more evidence of outcome benefit as first line therapy.
Again, I think these guidelines are an oversimplification and are not sufficient to guide individualized therapy.
DR. IZZO: Let’s close with some general discussion of whether the concept of the difficult-to-treat patient is useful and who might fill this definition.
DR. MOSER: It’s not necessarily related to having a comorbidity. You can have a diabetic hypertensive person with hyperlipidemia who responds very well to antihypertensive therapy. We’ve defined some patients as resistant, which may not be true. They may be difficult to treat. For example, just adding a thiazide-type diuretic to other drugs or increasing the dose of a thiazide-type diuretic will often convert a so-called “resistant patient” into a responsive patient.
That’s why I have supported JNC 7 and other guidelines that recommend starting with 2 drugs, either as 2 pills or in a single-pill combination when BP exceeds 160/100 mm Hg. One of the 2 drugs probably should be an RAS inhibitor, but the other most certainly should be a thiazide-type diuretic or perhaps a CCB.12
There are a lot of people with few other risk factors who are very difficult to control. One of the fallouts of the JNC 8 recommendations is that we may undertreat individuals over the age of 60, but that also means there will be less “resistant hypertension.”
DR. IZZO: When considering resistant hypertension, Dr. Moser suggested combination therapy. Dr. Gradman, you have had an interest in this area.
DR. GRADMAN: This is an important issue that has not really been addressed adequately in the guidelines. We know that combination therapy is required in upwards of 75% of patients using older BP targets.13 We also know that if you start people on combination therapy, you achieve target BP more rapidly and in a greater proportion of patients.
As to initial combination therapy versus the step-care type approach, either alternative is mentioned in JNC 8, but I don’t think any of the new guidelines have addressed the issue fully and no outcome studies have compared initial combination therapy versus initial monotherapy.
But the bottom line is that combination therapy is needed in the vast majority of patients although the percentage will be decreased if the newer, less aggressive BP targets are adopted. In my opinion, it should be started in almost everyone likely to eventually need more than 1 drug to achieve target BP. First-dose adverse effects, particularly hypotension, are very uncommon with 2- or 3-drug single-pill combinations that contain thiazide-type diuretics, ARBs, or CCBs. I would probably not use combinations as initial therapy in very elderly or frail patients.
DR. IZZO: I rarely use monotherapy anymore. Let me return to something that I touched on before: race as a decision point.
DR. BASILE: Well, I can understand why you’re against it, Dr. Izzo, because of the heterogeneity of how we define race. The white/black definition is certainly a simplistic approach given the way our genetics are so often mixed in today’s populations.
Both JNC 8 and the ASH/ISH document should, at least, be commended for pointing out to the clinician that if you’re looking for BP reduction, the CCB or the thiazide-type diuretic will give you more BP reduction in blacks in general than that achieved with an RAS blocker.
There are many African-American patients who are not prescribed a thiazide or a CCB as part of their cocktail. The big mistake is that these patients are considered resistant or refractory, depending on how many drugs they’re on. So I would at least point out, in line with JNC 8 and the ASH/ISH recommendations, that in the black patient, regardless of age, a CCB or a thiazide should be prescribed for BP reduction.
DR. IZZO: I think that’s a valid point. And just to summarize, the data show clearly that in an African-American population, you get about the same degree of BP reduction by using either a thiazide-type diuretic or CCB, and you do tend to have a more limited response to RAS blockers. The reverse could be stated for whites. But then again, if you use a thiazide-type diuretic and an RAS blocker together, the race issue is moot.
DR. MOSER: For years we have been studying black patients around the world, and there’s no question that there is a different response. I also want to return to something mentioned earlier: we are losing sight of the value of so-called “experts.” Simple guidelines work for the vast majority of patients. The complicated patient should probably be referred to an expert.
DR IZZO: Are there other issues when it comes to managing the hard-to-treat patient?
DR. GRADMAN: There are many reasons why a patient may be difficult to treat. Some may truly not respond to drugs but others have hypertension in the office and not at home. They may be difficult to treat because they don’t take their medications for various reasons. The other thing, of course, is to ask whether patients are taking any interfering substances like nonsteroidal antiinflammatory drugs. Most often, if you have people who are truly poorly responsive to antihypertensive therapy, it is worth reviewing whether adequate doses of preferred agents (RAS blockers, thiazide-type diuretics, and CCBs) have been used.
Most people these days also use aldosterone antagonists as the fourth drug, recognizing the danger of hyperkalemia particularly in patients receiving renin-angiotensin aldosterone system inhibitors. If patients have renal insufficiency, using a sufficient dose of thiazide-type diuretics is extremely important, and for patients with advanced renal disease, a loop diuretic is required. There may also be some intraclass differences among drugs, as between losartan and azilsartan.
DR. BASILE: I’m now running a resistant hypertension clinic, seeing only difficult-to-treat patients. As we saw in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), there is no question that the difficult-to-treat patient may be a little more likely to be black with left ventricular hypertrophy, CKD, obese, and elderly.
But the reality is there are patients in our practices that are called resistant that really only have white-coat hypertension and may have markedly reduced BPs when they’re out of the office. These are the same patients that complain of being periodically light headed or lethargic when their pressures are low outside of the office and often have minimal target organ disease with benign eyegrounds, no left ventricular hypertrophy on electrocardiogram, and minimal if any protein in the urine.
Another major issue is the use of inadequate doses of agents such as amlodipine when started at 2.5 mg daily and never up-titrating to the standard doses of 5 or 10 mg daily because of the concern of edema. I also find that replacing hydrochlorothiazide 25 mg with chlorthalidone at the same dose can improve BP control. And we have already mentioned the important role of spironolactone.
DR. MOSER: Let me emphasize that about half of the patients referred to as “resistant” respond when you increase the thiazide-type diuretic; this also seems to be true for the addition of spironolactone to hydrochlorothiazide. Combinations have a clear advantage in terms of a meaningful response.
DR. IZZO: It still begs the question to me of whether or not we’ve given enough guidance to well-meaning practitioners in this tougher-to-treat group of patients.
DR. GRADMAN: Let me point out the paper on resistant hypertension from the American Heart Association14 as a useful comprehensive reference, but perhaps we need a relatively simple document that could be used by practicing physicians who regularly treat these patients.
DR. BASILE: I would agree with Dr. Gradman that we need to continue to provide more information on the resistant patient.
DR. IZZO: Dr. Moser, you have the last word.
DR. MOSER: If you look at the general approach in JNC 8 and the algorithm in JNC 7, you’ll find a perfectly good and reasonable approach to the management of hypertension, including for the so-called resistant or difficult-to-treat patient. It seems physicians have been afraid to lower BP, especially in the elderly. This may be one of the reasons why JNC 8 recommends a target of 150 mm Hg and not to go below that. There’s an unfounded fear of the J-curve, of causing fainting or falling in patients, especially the elderly, that does not appear to be too much of a problem if BP is reduced gradually.15
It’s unlikely that we will cause much harm and may actually reduce cardiovascular events more in the elderly if we lower the goals to what we had before. But the JNC 8 algorithm is out there and probably will be followed by many physicians.
DR. IZZO: Thank you all very much for your valuable insights. The acid test, however, is what practitioners think and what they will do. We have recent insight into this area (Table). As is readily apparent, the opinion piece we call JNC 8 does not fully resonate with the majority of primary care providers or cardiologists. What will fill the need remains to be determined.
Disclosures: Joseph Izzo has been a consultant for Novartis and Bristol-Myers Squibb, has received a research grant from Forest Laboratories, and has received speakers’ honoraria from the American Society of Hypertension. Alan Gradman is a consultant for Daiichi-Sankyo, Novartis, Forest Laboratories, and Takeda. He is a member of the Speakers Bureau for Daiichi-Sankyo, Novartis, Forest Laboratories, Takeda, and Arbor. Over the past year, he has also received honoraria for lectures sponsored by The American Society of Hypertension and The American College of Cardiology. Jan Basile is a consultant for Daiichi-Sankyo, Forest, Arbor, Eli-Lilly, and Medtronic. He has received grant/research support from NHLBI (SPRINT). He is a member of the speakers’ bureau at Daiichi-Sankyo, Forest, and Arbor.
Addendum: The concerns raised during this discussion have been echoed by clinicians in the field. Cardiologists have indicated that they are waiting for yet another hypertension guideline proposed by the American Heart Association/American Society of Cardiology for 2014–2015 (Figure). 16 Clearly the fractionation continues.
FoxP2 Media LLC is the publisher of The Medical Roundtable.