From the Department of Neurology, Duke University Medical Center, Durham, NC (Dr. McFarlin), the Department of Psychosocial Oncology and Palliative Care, Dana-Farber Cancer Institute, Boston, MA (Dr. Tulsky), Harborview Medical Center, University of Washington, Seattle, WA (Dr. Back), and Department of Medicine, University of Pittsburgh, Pittsburgh, PA (Dr. Arnold).
Abstract
- Objective: To describe the use of a cognitive map for navigating family meetings with surrogate decision makers of patients in an intensive care unit.
- Methods: Descriptive report and discussion using an illustrative case to outline the steps in the cognitive map.
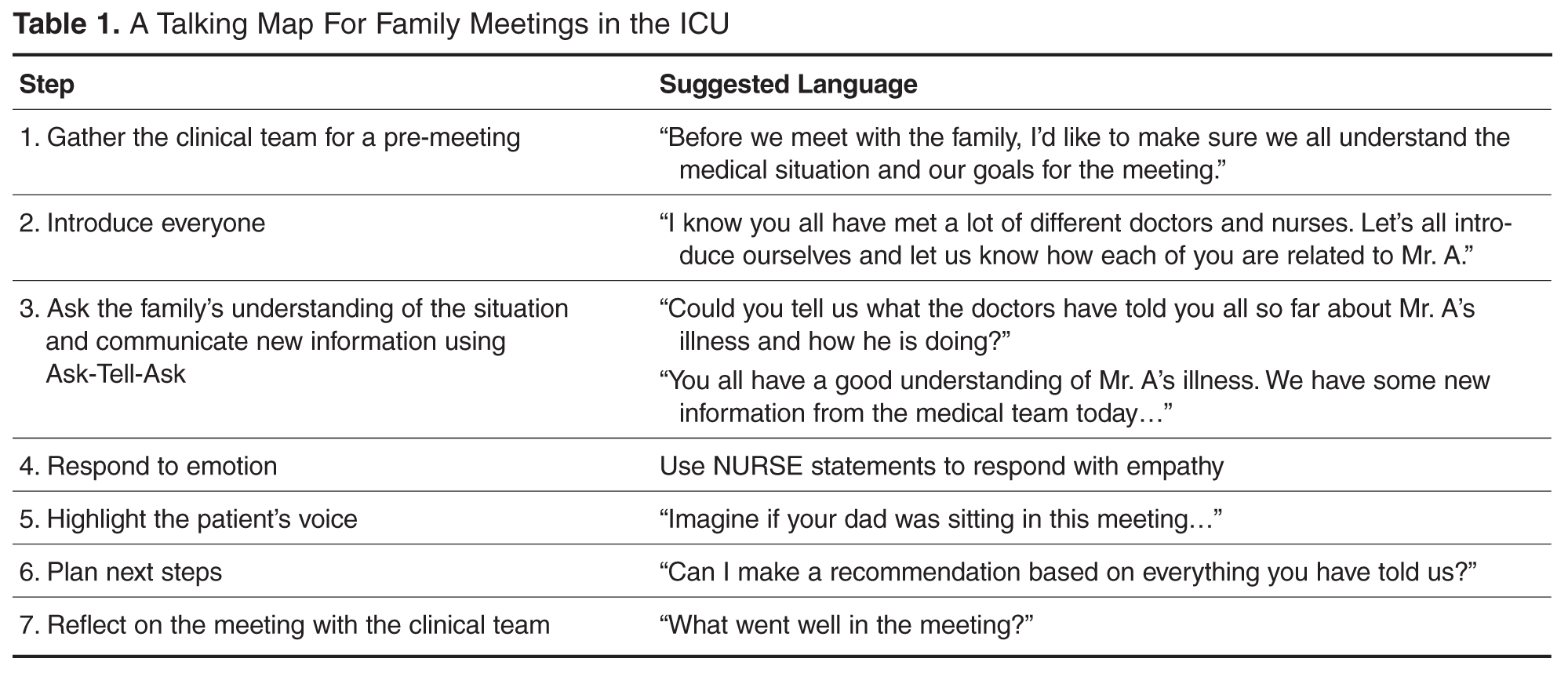
- Results: The use of cognitive maps has improved the ability of physicians to efficiently perform a specific communication skill. During a “goals of care” conversation, the cognitive map follows these steps: (1) Gather the clinical team for a pre-meeting, (2) Introduce everyone, (3) Use the “ask-tell-ask” strategy to communicate information, (4) Respond to emotion, (5) Highlight the patient’s voice, (6) Plan next steps, (7) Reflect on the meeting with the team. Providing this map of key communication skills will help faculty teach learners the core components of a family meeting.
- Conclusion: Practicing the behaviors demonstrated in the cognitive map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Key words: intensive care unit; communication; family meeting; critical illness; decision making; end of life care.
Family members of patients in the ICU value high-quality communication with the medical team. In fact, family members report that physicians’ communication skills are often more important than their medical skills [1]. Multiple professional societies, including the American Thoracic Society and the Society of Critical Care Medicine, define communication with families as a key component of high-quality critical care. Effective physician-patient communication improves measureable outcomes including decreased ICU length of stay [2] and may reduce distress amongst patients’ families [3]. The American College of Chest Physicians position statement on Palliative and End-of-Life Care for Patients with Cardiopulmonary Diseases urges physicians to develop curricula that incorporate interpersonal communication skills into training [4].
Unfortunately, such high-quality communication is not the norm. Surrogate decision makers are often displeased with the frequency of communication, the limited availability of attending physicians, and report feeling excluded from discussions [5]. When family meetings do occur, surrogate decision makers report inadequate understanding of diagnosis, prognosis, and treatment plans [6].
Physicians also find family meetings difficult. Intensivists worry that high-quality family meetings are time consuming and difficult to do in a busy ICU [7]. Critical care fellows report not feeling adequately trained to conduct family meetings [8]. It makes sense that untrained clinicians would want to avoid a conversation that is emotionally charged, particularly if one is unsure how to respond effectively.