Study Definitions
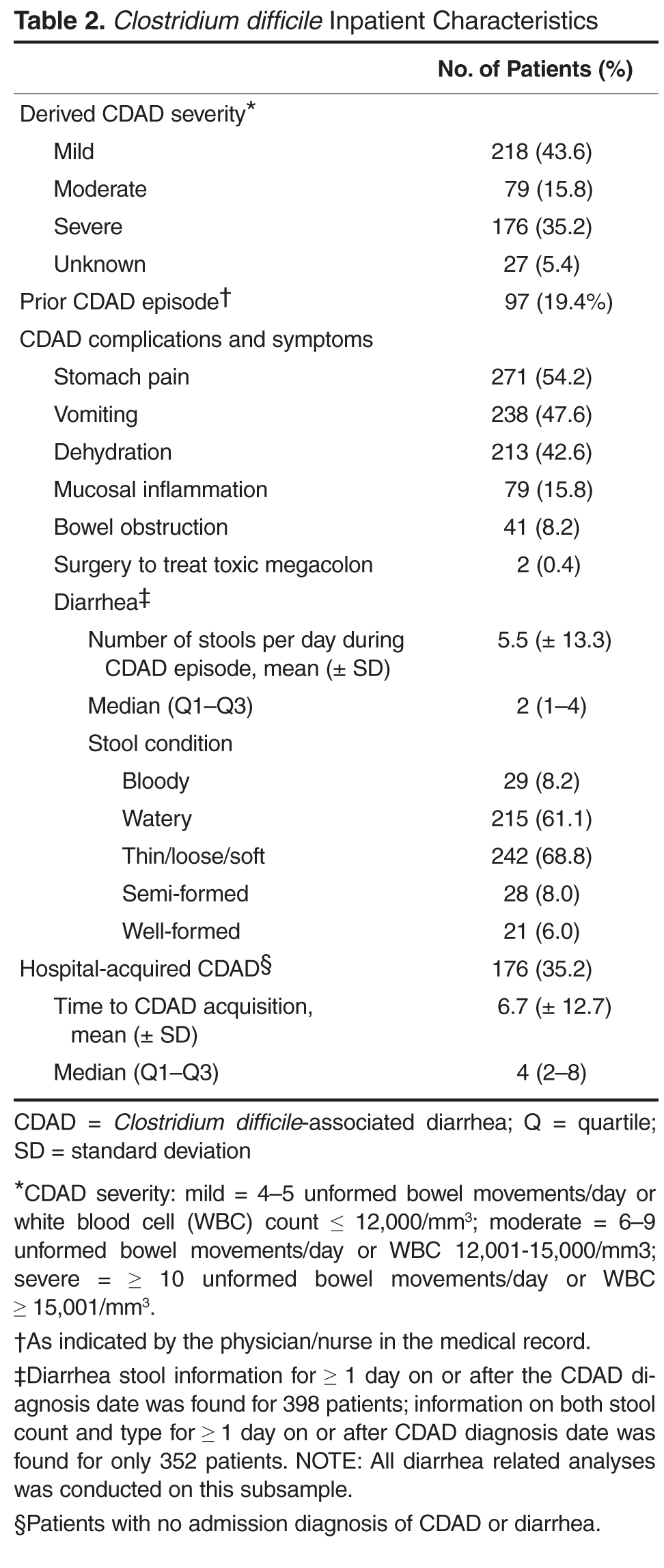
Diarrhea was defined as 3 or more unformed (includes bloody, watery, thin, loose, soft, and/or unformed stool) bowel movements per day.CDAD severity was classified as mild (4–5 unformed bowel movements per day or WBC ≤ 2000/mm 3); moderate (6–9 unformed bowel movements per day or WBC between 12,001/mm 3 and 15,000/mm 3); or severe (≥10 unformed bowel movements per day or WBC ≥15,001/mm 3) [12,13]. Diarrhea was considered to be resolved when the patient had no more than 3 unformed stools for 2 consecutive days and lasting until treatment was completed, with no additional therapy required for CDAD as of the second day after the end of the course of therapy [2,14].CDAD episode was defined as the duration from the date of the CDAD diagnosis or confirmation (whichever occurred first), to the date of diarrhea resolution (where documented) or discharge date.
Cost Measures
The total hospital health plan paid costs for the entire inpatient episode (includes treatment costs, diagnostics, services provided, etc.) were estimated using medical claims present in the database and pertaining to the hospitalization from where medical records were abstracted. Then the proportionate amount for the duration of the CDAD episode (from CDAD diagnosis to the diarrhea resolution date or the discharge date in cases where the resolution date could not be ascertained) was calculated to estimate the average CDAD associated in-hospital costs.
Analysis
Means (± standard deviation [SD]), medians (interquartile range Q1 to Q3), and relative frequencies were calculated for continuous and categorical data, respectively. This analysis was descriptive in nature; hence, no statistical tests to determine significance were conducted.
Results
We had a 55.3% success rate in obtaining the medical records from the contacted hospitals with refusal to participate/consent by the hospital in question being the most frequent reason for failure in 3 out of 4 cases. An additional attrition of 39.3% was observed among the medical records received, with absence of a MAR form (23.9%) and confirmatory CDAD diagnosis or note (9.1%) being the most frequent criteria for discarding an available record prior to abstraction (Figure).
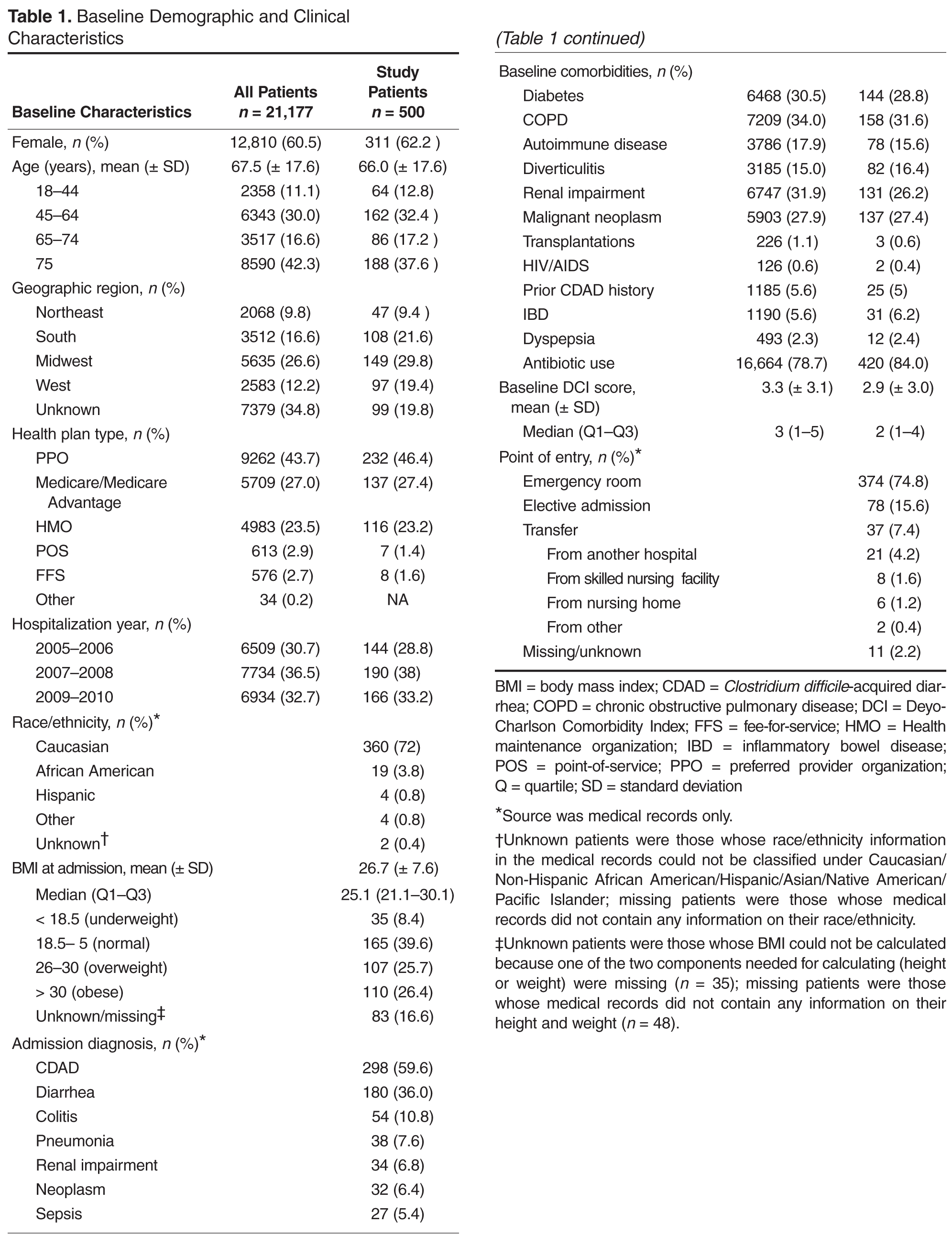
Patient Characteristics
CDAD Characteristics and Complications
Using a derived definition of severity, most CDAD cases were classified either as