Colorectal Cancer: Screening and Surveillance Recommendations
Journal of Clinical Outcomes Management. 2015 March;22(3)
References
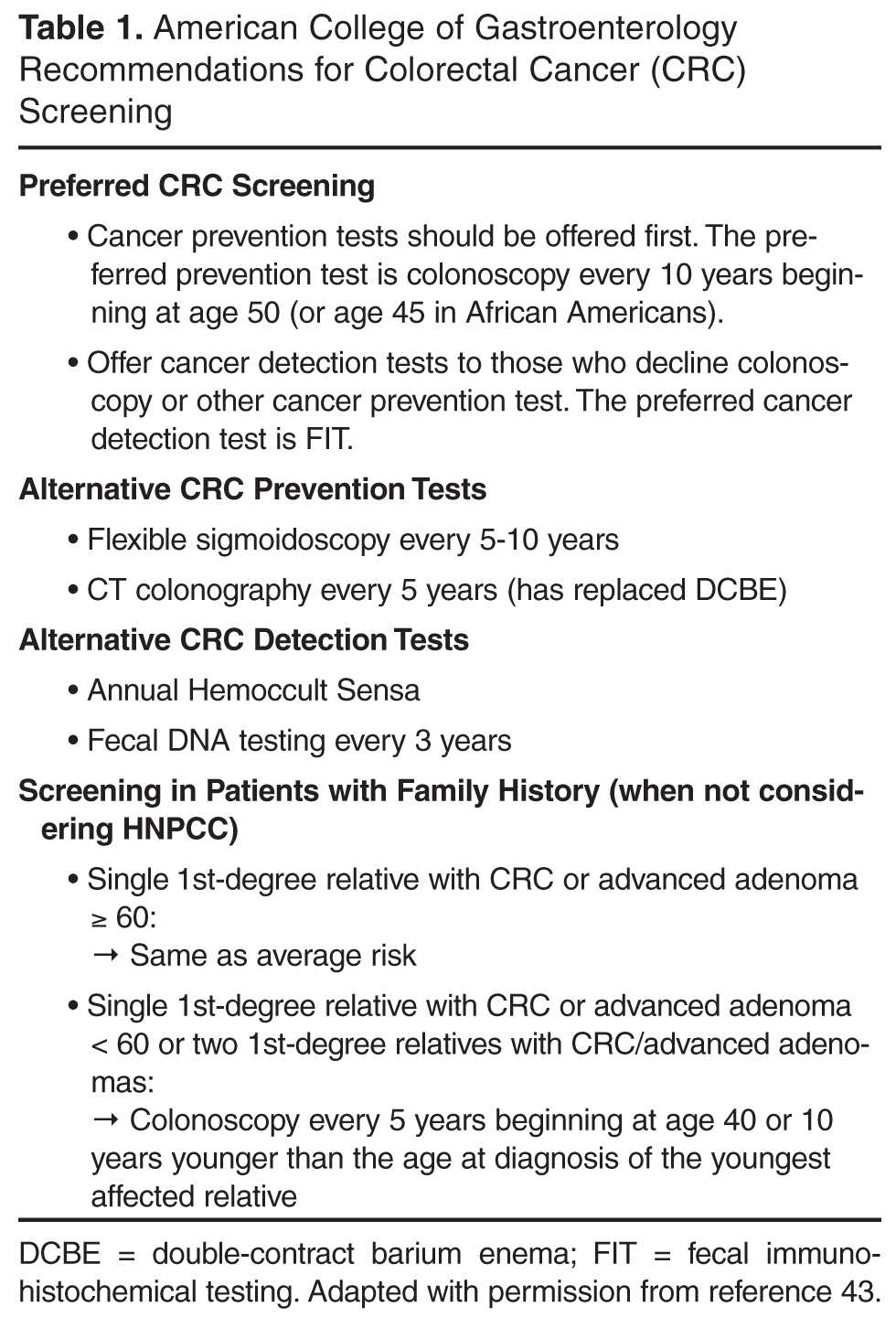
At this time, colonoscopy every 10 years, beginning at age 50, is the American College of Gastroenterology-preferred CRC screening strategy [43]. In cases when patients are unwilling to undergo colonoscopy for screening purposes, patients should be offered flexible sigmoidoscopy every 5-10 years, a computed tomography (CT) colonography every 5 years, or fecal immunohistochemical test (FIT) [43] ( Table 1 ). The US Preventive Services Task Force (USPSTF) recommends screening for colorectal cancer using fecal occult blood testing, sigmoidoscopy, or colonoscopy in adults, beginning at age 50 years and continuing until age 75 years [44].
Stool-Based Testing
Stool blood tests are conventionally known as fecal occult blood tests (FOBT) because they are designed to detect the presence of occult blood in stool. FOBT falls into 2 primary categories based on the detected analyte: guaiac-based and FIT. Blood in the stool is a nonspecific finding but may originate from CRC or larger (> 1 to 2 cm) polyps. Because small adenomatous polyps do not tend to bleed and bleeding from cancers or large polyps may be intermittent or undetectable in a single sample of stool, the proper use of stool blood tests requires annual testing that consists of collecting specimens (2 or 3, depending on the product) from consecutive bowel movements [45–47].
Guaiac-based FOBT
Guaiac-based FOBT (gFOBT) is the most common stool blood test for CRC screening and the only CRC screening test for which there is evidence of efficacy from randomized controlled trials [11]. The usual gFOBT protocol consists of collecting 2 samples from each of 3 consecutive bowel movements at home. Prior to testing with a sensitive guaiac-based test, individuals usually will be instructed to avoid aspirin and other NSAIDs, vitamin C, red meat, poultry, fish, and some raw vegetables because of diet-test interactions that can increase the risk of both false-positive and false-negative (specifically, vitamin C) results [48]. Collection of all 3 samples is important because test sensitivity improves with each additional stool sample [41]. Three large randomized controlled trials with gFOBT have demonstrated that screened patients have cancers detected at an early and more curable stage than unscreened patients. Over time (8 to 13 years), each of the trials demonstrated significant reductions in CRC mortality of 15% to 33% [49–51]. However, the reported sensitivity of a single gFOBT varies considerably [52].
FIT
FIT has several technological advantages when compared with gFOBT. FIT detects human globin, a protein that along with heme constitutes human hemoglobin. Thus, FIT is more specific for human blood than guaiac-based tests, which rely on detection of peroxidase in human blood and also react to the peroxidase that is present in dietary constituents such as rare red meat, cruciferous vegetables, and some fruits [53]. Furthermore, unlike gFOBT, FIT is not subject to false-negative results in the presence of high-dose vitamin C supplements, which block the peroxidase reaction. In addition, because globin is degraded by digestive enzymes in the upper gastrointestinal tract, FIT is also more specific for lower gastrointestinal bleeding, thus improving the specificity for CRC. Finally, the sample collection process for patients for some variants of FIT are less demanding than gFOBT, requiring fewer samples or less direct handling of stool, which may increase FIT’s appeal. Although FIT has superior performance characteristics when compared with older guaiac-based Hemoccult II cards [54–56], the spectrum of benefits, limitations, and harms is similar to a gFOBT with high sensitivity [41]. As for adherence with FIT, there were 10% and 12% gains in adherence with FIT in the first 2 randomized controlled trials comparing FIT with guaiac-based testing [57,58]. Therefore, FIT is preferred over Hemoccult Sensa and is the preferred annual cancer detection test when colonoscopy is not an option [43]. The American College of Gastroenterology supports the joint guideline recommendation [11] that older guaiac-based fecal occult blood testing be abandoned as a method for CRC screening.