Colorectal Cancer: Screening and Surveillance Recommendations
Journal of Clinical Outcomes Management. 2015 March;22(3)
References
Patients who meet the Bethesda criteria for HNPCC [65] can be screened by 2 different mechanisms. One is a DNA-based test for microsatellite instability of either the patient’s or a family member’s tumor. The other mechanism is to assess by immunohistochemical staining for evidence of mismatch repair proteins (eg, MLH1, MSH2, MSH6). In those patients in whom deleterious mutations are found, the affected individual should undergo colonoscopy every 2 years beginning at age 20 to 25 years until age 40 years, then annually thereafter [43]. If genetic testing is negative (ie, no deleterious mutation is found), but the patient is still felt to clinically have Lynch syndrome, then they should still be surveyed in the same way.
Case Continued
The physician recommends colonoscopy as the screening modality as it is the most efficient and accurate way of finding precancerous lesions and the most effective way of preventing CRC by removing precancerous lesions. He also explains that because the patient’s father developed CRC after the age of 60, this does not place the patient in a higher risk category and he can follow screening recommendations for “average-risk” individuals.
Screening
The patient undergoes colonoscopy. Two 5-mm adenomas in the transverse colon are detected and removed.
When should he have a repeat colonoscopy?
Surveillance Intervals
New data have recently emerged on the risk of interval cancer after colonoscopy. The overall rate of interval cancer is estimated to be 1.1–2.7 per 1000 person-years of follow-up. There are several reasons that may account for why patients develop interval cancers: (1) important lesions may be missed at baseline colonoscopy, (2) adenomas may be incompletely removed at the time of baseline colonoscopy, and (3) interval CRC may be biologically different or more aggressive than prevalent CRC. In order to minimize the risk of interval cancer development, it is important to perform a high-quality baseline screening colonoscopy examination as this is associated with lowering the risk of interval cancer [66]. A high-quality colonoscopy entails completion of the procedure to the cecum (with photodocumentation of the appendiceal orifice and ileocecal valve) with careful inspection of folds including adequate bowel cleanliness and a withdrawal time > 6 minutes.
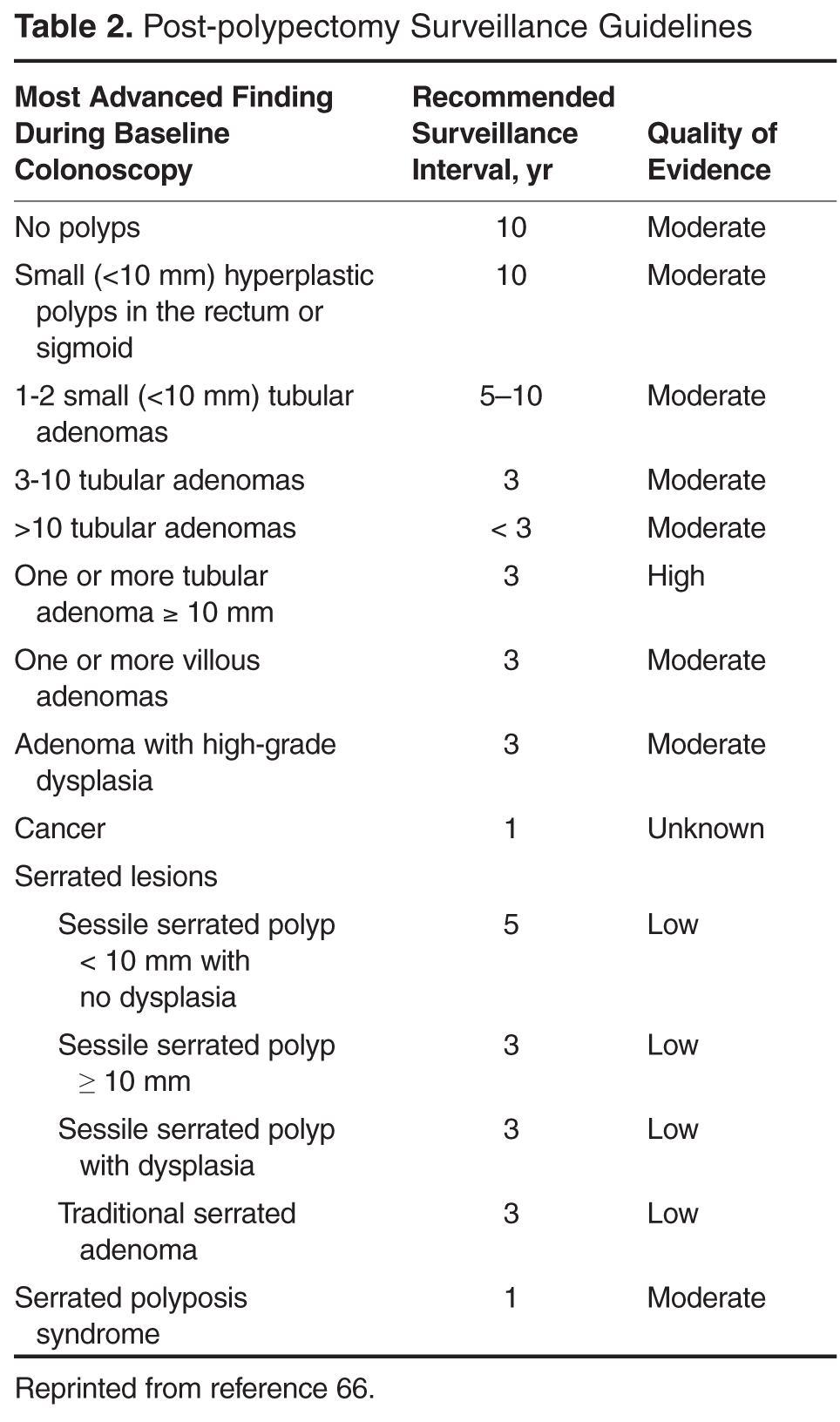
The MSTF guidelines for surveillance after screening and polypectomy were published in 2006 [67], with an update in 2012 [66]. Their recommendations on surveillance colonoscopy are based on the predication that the initial colonoscopy is high quality and are summarized in Table 2 and discussed below.
Baseline Colonoscopy Findings
No Polyps
Several prospective observational studies in different populations have shown that the risk of advanced adenomas within 5 years after negative findings on colonoscopy is low (1.3%–2.4%) relative to the rate on initial screening examination (4%–10%) [68–73]. In these studies, interval cancers were rare within 5 years. A sigmoidoscopy randomized controlled trial performed in the United Kingdom demonstrated a reduction in CRC incidence and mortality at 10 years in patients who received one-time sigmoidoscopy compared with controls—a benefit limited to the distal colon [46]. This is the first randomized study to show the effectiveness of endoscopic screening, an effect that appears to have at least a 10-year duration [74]. Thus, in patients who have a baseline colonoscopic evaluation without any adenomas or polyps and are average-risk individuals, the recommendation for the next examination is in 10 years [66].