Early Recognition: The Rate-Limiting Step to Quality Care for Severe Sepsis Patients in the Emergency Department
Journal of Clinical Outcomes Management. 2015 May;22(5)
References
Of importance to the ED clinician, an episode of sepsis has long-term effects on cognitive and physical function, quality-of-life, and survival [10,11]. Post-discharge, approximately one-quarter of sepsis survivors will be readmitted within 30 days [12–14]. In as many as half of these instances, another life-threatening infection is the cause for readmission, making the past medical history, including a detailed accounting of recent episodes of sepsis, an important part of the initial ED evaluation [12]. Furthermore, severe sepsis survivors spend a large proportion of their time following discharge within a health care facility, and will frequently present to the ED with an acute condition from such an environment. Important factors for predicting readmission after a sepsis hospitalization include patient age, severity of illness, hospital length of stay, and the need for intensive care during the initial hospitalization [12–14].
Principles of Effective Sepsis Management
The principles of effective sepsis management begin with early identification in the pre-hospital setting, at triage, or when a patient begins to decompensate in the hospital. After the point of initial recognition, core principles include risk stratification, timely and appropriate antimicrobial administration, initial intravenous fluid boluses and ongoing resuscitation guided by physical examination and objective resuscitation end-points [4,5]. These practices have been operationalized in the care bundles of the Surviving Sepsis Campaign Guidelines [4]. Within 3 hours, the resuscitation bundle includes measuring serum lactate to risk stratify patients, obtaining blood cultures, administering broad-spectrum antibiotics, and administering 30 mL/kg crystalloid in patients with hypotension or hyperlactatemia [4]. The 6-hour bundle expands upon these initial measures and includes additional management recommendations based on resuscitation end-points.
As effective management is predicated on timely recognition, an understanding of the impact of delayed recognition is essential to provide optimal care for the severe sepsis patient in the ED. Decades of research has revealed that certain markers predict adverse outcomes, including transition to septic shock and death, as do delayed processes of care. Importantly, while early quantitative resuscitation was demonstrated to improve outcomes in a meta-analysis, there was no demonstrable benefit when resuscitation was initiated late (> 24 hours) in the course in the ICU (odds ratio of death, 1.16 [95% confidence interval, 0.60–2.22]) [15].
Strategies To Improve Recognition
Pre-Hospital Environment
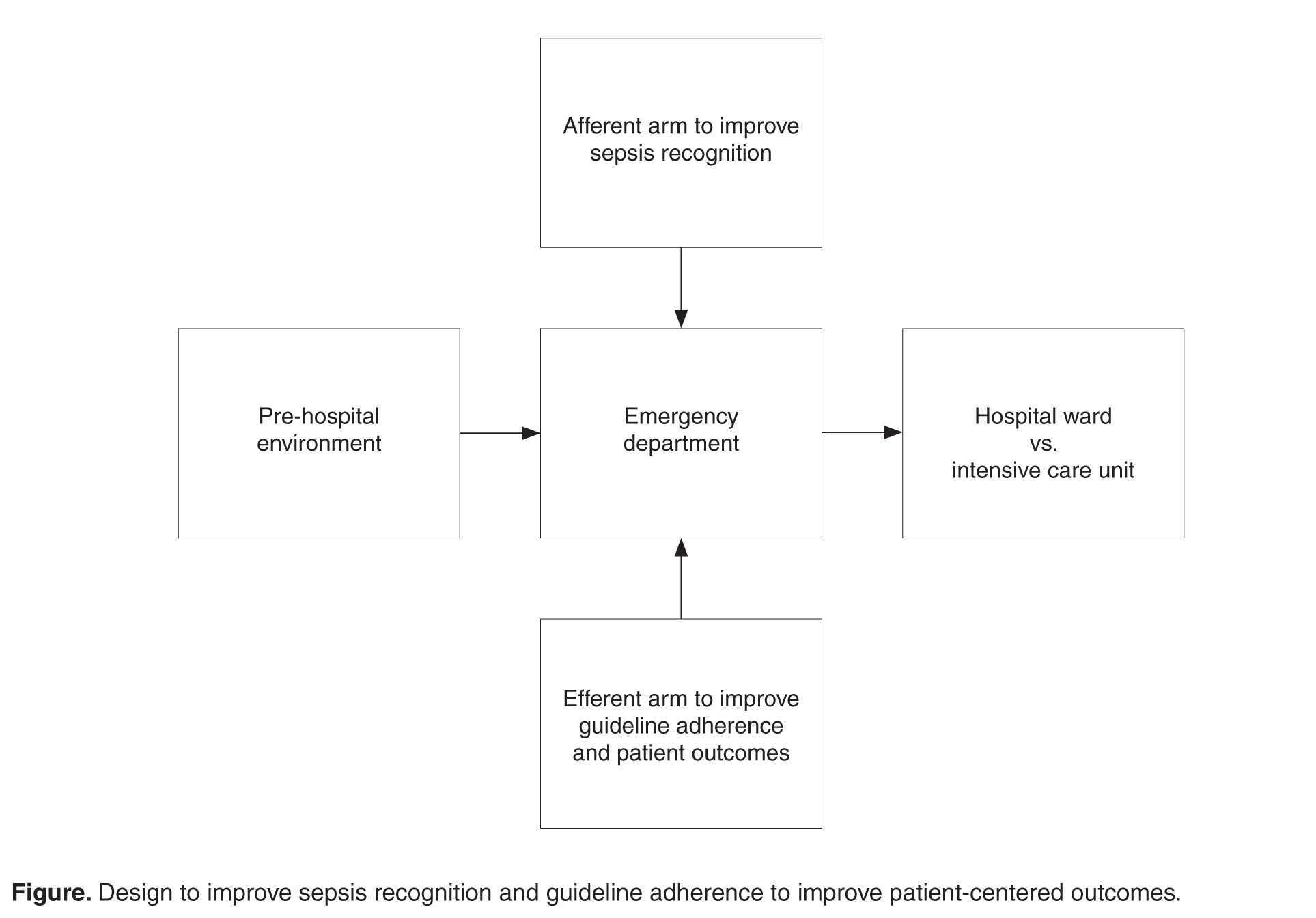
As many as 40% of severe sepsis cases admitted to the hospital from the ED will present to the ED via emergency medical services (EMS) transport, and this rate appears to be increasing over time [16]. Thus, efforts to improve identification and risk-stratification of potential cases of severe sepsis should begin in the pre-hospital environment. These EMS encounters frequently exceed 45 minutes [16], pre-hospital interventions appear to be uncommon [16,17], and establishment of intravenous access paired with fluid resuscitation in the pre-hospital environment may improve survival [18]. Further, when EMS providers recognize sepsis, ED care processes (eg, time to antibiotics, protocol-directed resus-citation) are improved, with shorter time to antibiotics and initiation of early goal-directed therapy (EGDT) [19] and a trend towards achieving goal mean arterial pressure earlier [17]. In sum, while further investigation is required to facilitate this transition, efforts to improve sepsis outcomes should also include the interface between the pre-hospital environment and the ED ( Figure