Early Recognition: The Rate-Limiting Step to Quality Care for Severe Sepsis Patients in the Emergency Department
Journal of Clinical Outcomes Management. 2015 May;22(5)
References
).
From EMS to ED Triage
Borrowing the principle “time equals tissue” from a variety of time sensitive conditions (eg, myocardial infarction management [“time equals muscle”] and stroke care [“time equals brain”]), clinicians and researchers have realized that expedited recognition of severe sepsis patients begins at the time of initial contact with the health care system. For severe sepsis patients, clinicians need to think “time equals organ function.” Given the frequency with which sepsis patients arrive to the ED via EMS, effective communication between EMS and ED providers could be leveraged to prepare the ED team to provide timely care for the sepsis patient via a “sepsis alert.” While confirmation of its applicability to sepsis care is required in the absence of a regionalized network of sepsis centers, the rationale is based on the experience of the effectiveness of trauma and stroke alert systems [20–22]. For patients not recognized as potentially being infected by EMS providers during transport, repeat vital signs during ED triage can be screened to identify patients exhibiting signs of the systemic inflammatory response syndrome (SIRS) [4,23]. The same principles of effective communication apply for patients being sent from medical clinics to the ED for evaluation and treatment of potential severe sepsis. For patients arriving independent of EMS, focused triage and initial vital signs are the starting point for identifying severe sepsis at the most proximal phase of entry into the health care system.
Vital Signs and SIRS Criteria in the ED
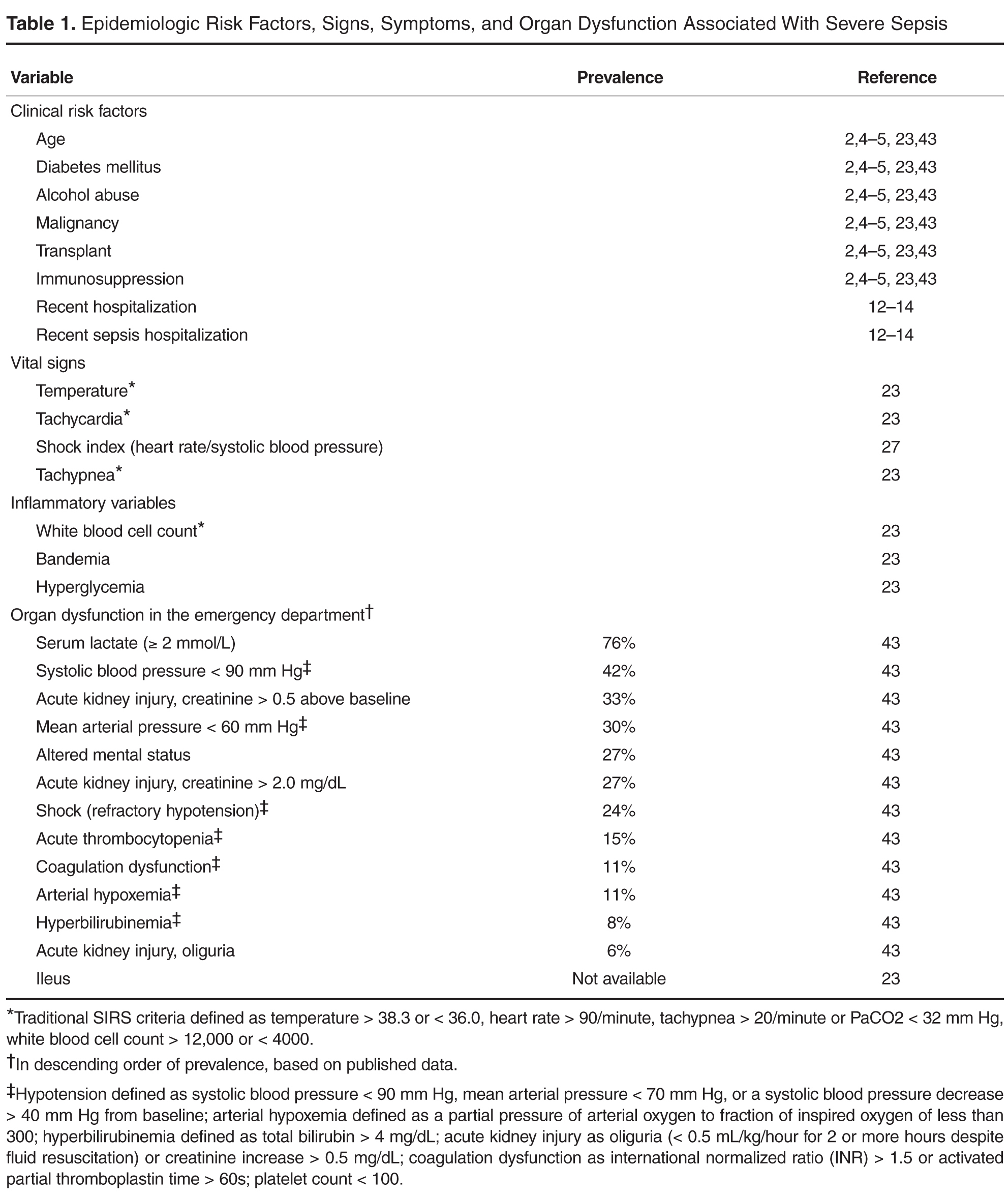
The vast majority of patients who are hypotensive in triage are expedited to a treatment room and early resuscitation is begun. However, these patients represent a minority of severe sepsis patients seen in triage; therefore, all available data need to be analyzed to capture the highest percentage of severe sepsis patients. Acknowledging that SIRS criteria are not specific for sepsis [24], will miss as many as 1 out of 8 patients initially [25], and may not predict mortality [26], their presence is nonetheless characteristic of sepsis. As such, identifying the presence of SIRS at triage, or during the ED stay via serial vital signs, facilitates sepsis recognition, as do strategies that leverage routine vital signs to calculate predictors of instability including the shock index (heart rate/systolic blood pressure), where a shock index ≥ 0.7 has been associated with illness severity [27]. An increased respiratory rate has been demonstrated to identify risk for transfer from a floor bed to the ICU within 24 hours of ED admission [28]. Further, clinical manifestations of sepsis, including end-organ dysfunction, are protean, and patients frequently present with nonspecific, constitutional symptoms (eg, weakness, malaise, fever, chills, nausea) that could reflect one of many diseases ( Table 1 ).
The Afferent Arm: Multimodal Screening Strategies
While institutional practice improvement initiatives to facilitate sepsis recognition and care should incorporate educational strategies, led by champions with expertise in sepsis, the complex presentation of sepsis requires multimodal approaches [29]. These multimodal approaches, beginning at the time of ED triage, should be designed to harness information technology to screen patients to improve severe sepsis recognition (the afferent arm) and to utilize structures and processes of care efficiently and effectively (the efferent arm) to guide severe sepsis management according to sepsis-care bundles espoused by guidelines (Figure) [4].