Evidence-based Management of Newly Diagnosed Chronic Lymphocytic Leukemia
Journal of Clinical Outcomes Management. 2014 April;21(4)
References
summarizes the differences between MBL, CLL, and SLL.
Care should be taken to exclude other malignancies with a similar morphology. Leukemic phase mantle cell lymphoma, other low grade lymphomas, and hairy cell leukemia are commonly mistaken for CLL. Immunophenotyping and cytogenetics are usually sufficient to differentiate these. Testing for a balanced translocation involving chromosomes 11 and 14 to exclude mantle cell lymphoma can be helpful, as both CLL and mantle cell lymphoma can appear morphologically similar and share immunophenotypic features (CD5+/CD19+).
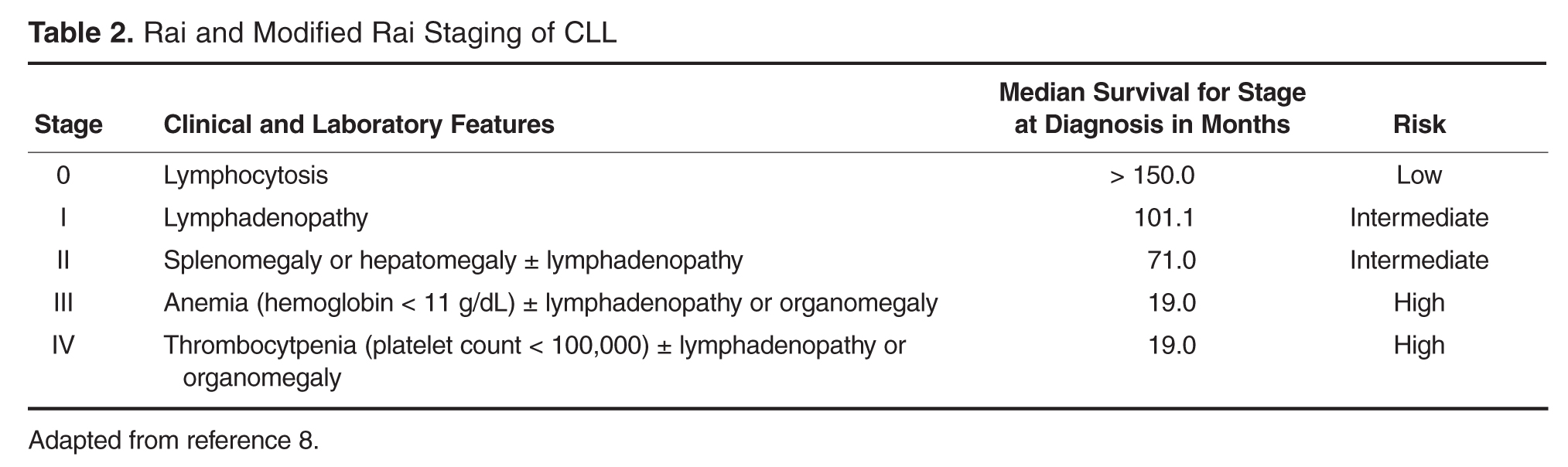
Staging for CLL is based on clinical exam and peripheral blood counts. Stage increases with the presence of lymph node or organ involvement on exam and the presence of associated anemia or thrombocytopenia. There are 2 distinct but similar staging systems in routine use: Rai and Binet. Both systems have prognostic significance, but the Rai system is more commonly used in the United States [8–10]. Table 2 presents the Rai staging system. For purposes of staging, no distinction is made between autoimmune cytopenias and those due to marrow infiltration [8]. The traditional Rai staging can be further refined into 3 risk groups with similar survival experience. Imaging with CT scans can be helpful for the evaluation of individual patients but has been found to be of limited benefit in routine evaluation. CT imaging is, however, recommended by the IWCLL to follow patients on clinical trial [11].
Case Continued
The patient’s peripheral blood is drawn for routine immunophenotyping as well as cytogenetic and molecular testing. When he returns to discuss the results 10 days later, he learns that peripheral blood immunophenotyping demonstrates a dim kappa restricted monoclonal population of B-cells that expressed CD19, CD20(dim), CD23, CD38, CD5, and CD43. The lymphocytes are negative for CD10, FMC7, and CD79b, consistent with a CLL immunophenotype. This patient fulfills diagnostic criteria for CLL and has Rai stage II or intermediate-risk disease. Interphase cytogenetic studies of the peripheral blood demonstrate deletions of chromosomes 11q22.3 and 13q14.3. The immunoglobulin heavy chain gene (IGHV) is unmutated.
• How can a CLL patient’s disease risk be characterized?
Historically, staging at diagnosis, pattern of bone marrow infiltration, and response to therapy were used to gauge prognosis. In more recent years, cytogenetic and molecular testing methods have been developed to augment risk stratification. Testing of prognostic significance that influences clinical management includes IGHV mutational status and interphase cytogenetics using FISH [3,12–14]. Expression of ZAP-70 and CD38 are both independent predictors of poorer prognosis in CLL but are not recommended for routine clinical use. Standardized methodology for the measurement of Zap-70 in particular limits the utility of that test in routine clinical practice [15]. Performed at diagnosis, a time when many patients are asymptomatic, cytogenetic testing with FISH and IGHV mutational analysis can predict time to first treatment and increasingly identify high-risk patients for whom investigational early intervention approaches may be considered [16]. While cytogenetic testing has utility at time of diagnosis, it should be considered necessary prior to deciding on the first-line treatment.
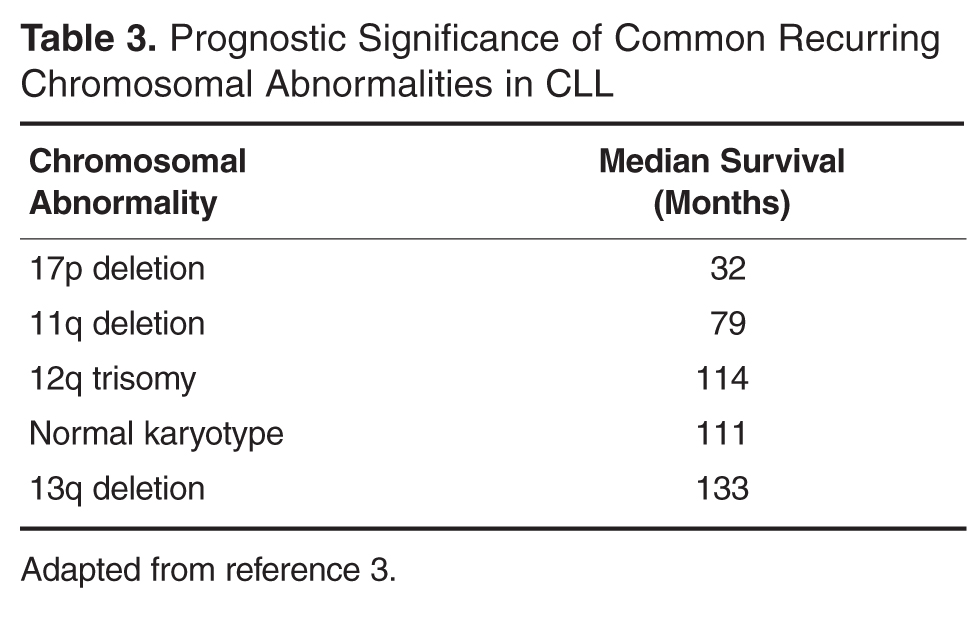
Due to the slow rate of cellular division, utility of conventional karyotype analysis is limited. Mitogen stimulated karyotype or interphase FISH is needed to more accurately assess for chromosomal abnormalities [3]. Using these methods, the most common recurrent chromosomal abnormalities are shown in Table 3