Interstitial cystitis (IC) is a debilitating disease that presents with a constellation of symptoms, including pain, urinary urgency, frequency, nocturia, and small voided volumes in the absence of other identifiable etiologies.1 The overall prevalence of IC among US women is between 2.7% and 6.5%—affecting approximately 3.3 to 7.9 million women2—and it results in substantial costs1,3 and impairments in health-related quality of life.4 Unfortunately, there is a lack of consensus on the pathophysiology and etiology of this prevalent and costly disorder. Thus, therapies are often empiric, with limited evidence and variable levels of improvement.5
There has been no clear evidence that bladder inflammation (cystitis) is involved in the etiology or pathophysiology of the condition. As a result, there has been a movement to rename it “bladder pain syndrome.” Current literature refers to the spectrum of symptoms as interstitial cystitis/bladder pain syndrome (IC/BPS).
Currently, the American Urological Association (AUA) defines IC/BPS as an unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder,
associated with lower urinary tract symptoms of more than 6 weeks’ duration, in the absence of infection or other identifiable causes.6 This is still a broad, clinical diagnosis that has significant overlap with other pain syndromes but allows for treatment to begin after a relatively short symptomatic period.7 Because gynecologists are frequently the main care providers for women, understanding the diagnosis and treatment options for IC/BPS is important to avoid delayed treatment in a difficult to diagnose population.
Recently, the AUA published an amendment to their 2011 management guidelines to provide direction to clinicians and patients regarding how to recognize IC/BPS, conduct valid diagnostic testing, and approach treatment with the goals of maximizing symptom control and patient quality of life.7
In this article, we review the AUA diagnostic and treatment algorithms and the results of recently published randomized trials comparing the efficacy of various treatment modalities for IC/BPS, including pentosoan polysulfate sodium (PPS; Elmiron, Janssen Pharmaceuticals, Titusville, New Jersey) and botulinum toxin (Botox, Allergan, Irvine, California) with hydrodistension.
Hanno PM, Erickson D, Moldwin R, Faraday MM; American Urological Association. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol. 2015;193(5):1545−1553.
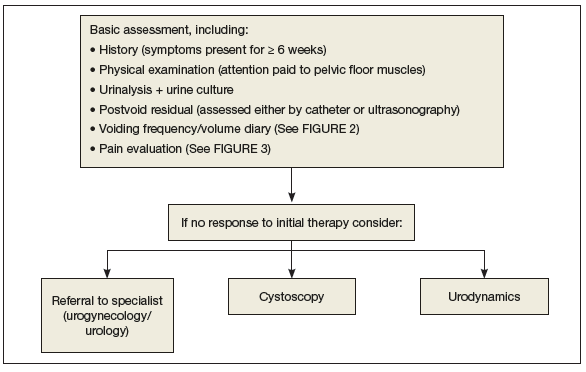
The diagnosis of IC/BPS can be challenging due to a wide spectrum of symptoms, physical examination findings, and clinical test responses. The AUA developed its diagnostic and treatment guidelines mostly based on expert opinion, but they do provide a framework to help clinicians determine whether or not treatment for IC/BPS is warranted. The primary principles for evaluation are presented in FIGURE 1.
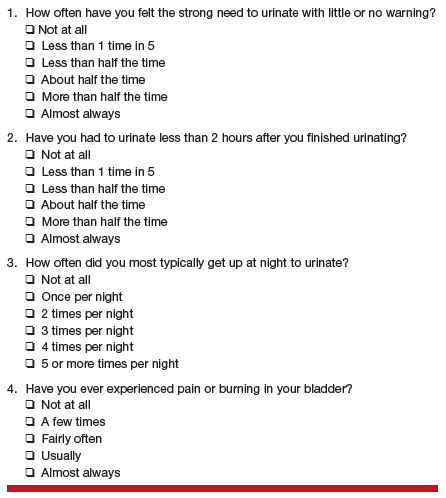
It is important to establish baseline voiding symptoms and pain levels with objective, validated instruments, including a voiding diary (FIGURE 2)9 and such patient questionnaires as the O’Leary Sant Interstitial Cystitis Index (ICSI; FIGURE 3).10 Characteristic IC/BPS voiding frequency is 10 or more times per day (to relieve pain, not to relieve a fear of wetting, which would be expected in a patient with overactive bladder).8 The ICSI questionnaire
should be used primarily to establish baseline symptoms, not as a diagnostic tool. A score higher than 8 has been used as inclusion criteria for therapeutic trials, however.11
FIGURE 2 Voiding diary9
|
FIGURE 3 O’Leary Sant Interstitial Cystitis Index10
|
It is unnecessary to primarily perform cystoscopy or urodynamics, as there are no agreed-upon diagnostic criteria for these modalities for IC/BPS. They may be considered, however, if the patient does not respond to first- and second-line therapies. Additionally, potassium sensitivity testing is painful and, in view of the paucity of benefits, the risk/benefit ratio is too high to recommend for clinical care.
The treatment for IC/BPS should start with more conservative therapy (including behavioral management and physical therapy). If symptom control is inadequate, other modalities should be employed. Behavioral modifications should include:
- local heat/cold over the bladder and perineum
- avoidance of foods and fluids that are known to be common irritants (such as coffee and citrus)
- trial of elimination diet
- bladder training with urge suppression techniques.
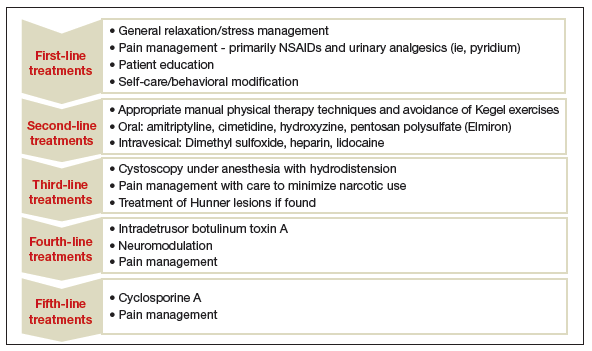
As noted in FIGURE 1, first make sure that patients do not have a urinary tract infection. If culture results are negative and other criteria fit, consider the diagnosis of IC/BPS and offer therapies as outlined in the treat‑
ment algorithm (FIGURE 4).7 Repeated
treatment for negative results of urine cultures in patients with frequency, urgency, and bladder pain can lead to unnecessary antibiotics and delayed treatment of IC/BPS.
Treatments in FIGURE 4 are ordered from most to least conservative, and initial treatment depends on symptom severity,
clinician judgment, and patient preference. If at any point in the patient’s care the diagnosis is questioned or treatments have been ineffective, referral to a specialist, including urogynecology or urology, may be appropriate.
Pain management is an important component at all levels of therapy, and pharmacologic pain management principles for
IC/BPS should be similar to those for management of other chronic pain states. Options primarily include nonsteroidal anti-
inflammatory drugs (NSAIDs) and urinary analgesics (pyridium). The use of narcotics presents the risks of tolerance and dependence. If their use is necessary, all narcotic prescriptions must come from a single source and should be used as a component of multimodality therapy to minimize narcotic use.