A description of two bipolar I disorder cases presents examples of the phenomenon of transient neutrophilia that occurred during admission into a state psychiatric hospital. A brief review of the mechanisms that may explain this hematologic response is included.
Background

Dr. Tim C. Taylor
In 1889, the U.S. territory of New Mexico established the New Mexico Insane Asylum, and it was known as such until 1955, when it became the State Hospital. In 1970, it became the Las Vegas Medical Center but changed its name in 2005 to the New Mexico Behavioral Health Institute (NMBHI), which services the entire state for inpatient and long-term care patients. On average, it accepts two admissions per day, of which two patients per month present with neutrophilia (white blood cell [WBC] count greater than 11,000), which resolves after 1-4 days in the hospital.
Case presentations
Case one. A 21-year-old Native American man presented with multiple psychiatric admissions for bipolar I disorder and major depression with suicidal ideation. He was brought into the local emergency department by police, who found him walking down the interstate highway trying to hitch a ride back to his native pueblo after a disagreement with a fellow resident at a local boarding home. He had discontinued his Seroquel and lithium 2 weeks earlier because he felt he no longer needed them and required medical clearance for admission.1 His presenting hemogram in the ED was normal except for an elevated WBC count of 20,000. His vital signs were normal except for tachycardia of 110 beats per minute. On exam the patient demonstrated a flat affect and anxiety but other than mild ingrown toenails and tachycardia, there were no abnormal findings.
He received a chest x-ray and abdominal computed tomography scan that were both normal, and the patient was cleared for admission. He was cooperative with staff and restarted his lithium. A repeat WBC at day 5 was 9,700.
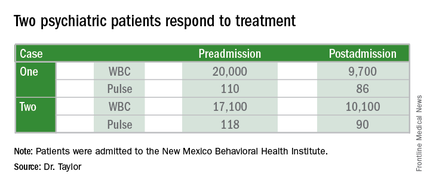
Case two. A 24-year-old white man with a history of bipolar I disorder and dependency on benzodiazepines and Ritalin was transferred from a distant county jail after 10 days of incarceration. He started screaming in his cell, praying, and perseverating that he “needed to kill himself,” which triggered his transfer to the NMBHI. His aggressive behavior upon arrival necessitated a transfer to the local ED for sedation and four-point restraints. He received Versed and Ativan IVP before allowing a blood collection, which revealed dehydration and a WBC count of 17,100. After 4 L of normal saline, his labs normalized with a WBC of 10,100, and he was admitted for a 7-day committal.
Discussion
Neutrophilia can result from granulocytes moving from pericapillary tissue margins into the circulating pool.2 It may occur in association with vigorous exercise, seizures, paroxysmal tachycardia, and adrenergic stress.3 The duration is fewer than 30 minutes and usually results in WBC counts of 15,000-20,000.4 Beta receptors on endothelial cells may mediate neutrophil adherence and release from marginal sites. A left shift is absent, because there is no change of the inflow of cells from the marrow.
In these two cases, a transient neutrophilia and tachycardia were observed. Neither case was febrile, and the platelet count remained normal. Both patients voluntarily stopped taking their lithium about 2 weeks before decompensating from bipolar I disorders. Stress was evident in both cases, one from walking on a cold December night after a disagreement, while the other patient in case two was highly agitated and aggressive requiring four-point restraints and intravenous sedation in the ED before admission to NMBHI. Past histories of psychiatric admissions were noted in both cases, and neither subject smoked tobacco – which can increase WBC by 25%-50% with the use of one-two packs per day, respectively.5
These two cases show that clinicians should consider stress in its many permutations to the long list of causes to explain elevated WBC, particularly in the ED. They also illustrate the power of antianxiety medications for some patients with acute mania who present to the ED.
References
1. J Emerg Med. 2012;43(5):866-70.
2. “Wintrobe’s Clinical Hematology,” Philadelphia: Lea & Febiger, 1981, p.1292.
3. “Diagnostic Hematology,” London: Springer, 2009, p. 324.
4. Gen Hosp Psychiatry. 2005;27(6):454-56.
5. Euro Heart J. 2003 Jul;24(14)1365-72.
Dr. Taylor is a staff physician affiliated with the New Mexico Behavioral Health Institute, New Mexico Department of Health, Santa Fe. He reports no financial disclosures or conflicts of interest. The author wishes to thank Dr. Dan Collins from the NMBHI for recommending that he research and write about this topic. In addition, document access was greatly aided by Lisa Apodaca and Mary Bunker, CNP, from the NMBHI, and Karen Ebler and Dr. Irwin Hoffman from Christus St. Vincent Hospital in Santa Fe. Finally, the following colleagues helped by proofreading the manuscript: Dr. Wendy Dimmette, Dr. Richard Nail, and Dr. Matt Streicherz. Eva Romero and Dr. Troy Jones provided useful historical documentation.