Fluvoxamine. Repetitive behaviors did not change—as measured with the CY-BOCS—when 18 children with autism received fluvoxamine, 1.5 mg/kg/day, in a 10-week prospective, open-label trial.8 Most patients (72%) reported at least one side effect, and 3 discontinued the SSRI because of behavioral activation. Ten completed the trial. Likewise in a randomized trial, children who received fluvoxamine experienced troublesome side effects and limited benefit.9
Compared with outcomes in children, fluvoxamine has shown greater efficacy in adults. In a 12-week, double-blind, placebo-controlled trial of 30 adults with autism, 8 of 15 treated with fluvoxamine (50 mg/d initially and titrated to 300 mg/d) were rated as responders, compared with none of 15 receiving placebo.
Repetitive behaviors and adaptive functioning improved significantly with fluvoxamine, as measured with the Yale-Brown Obsessive Compulsive Scale (YBOCS) and Vineland Adaptive Behavior Scale, respectively.10 The SSRI was well-tolerated, with only mild nausea and sedation reported.
Thus, fluvoxamine may be useful for treating repetitive behaviors but probably is not a first choice for children with autism. Results might be more favorable in children if fluvoxamine were available in doses <12.5 mg.
Citalopram. Open-label data support using citalopram in autism.11 In a retrospective chart review, 10 of 15 children (73%) were reported “much improved” with citalopram (mean dosage 16.9 mg/d [+/-12.1]), but the review did not specifically address repetitive behaviors. Two patients stopped taking the SSRI because of side effects; agitation, aggressiveness, sedation, and lip dyskinesia were reported.
The National Institutes of Health is sponsoring a multicenter trial of citalopram (starting dosage 2.5 mg/d, up to 20 mg/d) for repetitive behaviors in 144 children with autism, Results are expected in 2007 (see Related resources).
Escitalopram. Some early, open-label evidence suggests that escitalopram may be well-tolerated in autism, but its efficacy for treating repetitive behaviors has not been studied.
Sertraline. One of three reported open-label studies of sertraline in patients with autism measured repetitive behaviors.12 In this study, 42 adults with autism spectrum disorder were treated for 12 weeks with sertraline, 50 to 200 mg/d. One-half were rated “much improved”—mostly in aggressive and repetitive behaviors—with the CGI improvement scale. Sertraline was well-tolerated, although 3 patients dropped out because of persistent agitation.
No randomized trials have examined sertraline in autism.
Clinical recommendations
Family history of bipolar disorder guides our treatment of patients with an autism spectrum disorder and disabling repetitive behaviors (Algorithm).
Algorithm Suggested medications to treat repetitive behaviors in autism
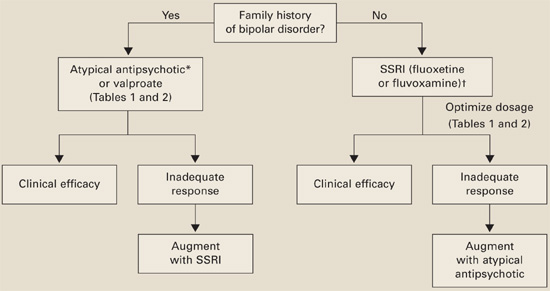
*Risperidone has the most evidence of efficacy, but aripiprazole may be useful for patients with weight-gain problems.
†For children, controlled data support using liquid fluoxetine, starting at 2.5 mg/d.Without bipolar history. SSRIs are usually first-line therapy (although patients with significant irritability and aggression may be an exception and require an atypical antipsychotic first).
If you reach the maximal SSRI dosage without a desired effect, consider adding an atypical (risperidone has the strongest supporting data) or valproate. If behavioral activation symptoms emerge and a lower dosage does not ameliorate them or reduces the clinical effect, consider switching to an atypical or valproate.
With bipolar history. Consider starting with an atypical or valproate; augment with an SSRI if needed.
Monitor for side effects with each medication (Table 2).
Table 2
Medication side effects and recommended monitoring
| Medication | Side effects | Recommended monitoring |
|---|---|---|
| Fluoxetine | Anxiety, insomnia, GI disturbance, appetite and weight changes, mania/hypomania activation, suicidal ideation | Observe closely when starting treatment and while increasing dosage |
| Fluvoxamine | Somnolence, nervousness, insomnia, agitation, GI disturbance, suicidal ideation | Observe closely when starting treatment and while increasing dosage |
| Risperidone | Drowsiness, weight gain, hyperglycemia, GI disturbance, extrapyramidal symptoms, neuroleptic malignant syndrome | Obtain metabolic profile, including serum glucose and lipids |
| Monitor for weight gain and clinical signs of extrapyramidal symptoms | ||
| Valproate | Rash, headaches, weight gain, ataxia, alopecia, GI disturbance, hyperammonemic encephalopathy, sedation, thrombocytopenia, polycystic ovary syndrome, pancreatitis, liver failure, teratogenic effects | CBC with platelets, liver function tests, valproate levels |
| Therapeutic blood levels: 50 to 120 mcg/mL |
Evidence for atypical antipsychotics
Atypicals have been used in autistic disorder to treat irritability and impulsive aggression. Risperidone also has been shown to reduce repetitive behaviors in a controlled trial.13 No evidence or only open-label trials support the use of other atypicals in patients with autism.
Risperidone’s side effects may include metabolic syndrome. No studies have examined lipid profiles and insulin resistance after risperidone treatment in patients with autism, but weight gain has been reported in the Research Units on Pediatric Psychopharmacology (RUPP) trial andothers.13-15 Carefully assess the risk-benefit ratio when you consider using risperidone to treat repetitive behaviors in patients with autism.
Atypical antipsychotics also may increase dyskinesia risk, although extrapyramidal symptoms (EPS) have not been reported in studies of patients with autism and repetitive behaviors. Because EPS could develop after clinical trials are completed, long-term naturalistic studies are needed to address this concern.