To begin monitoring Sammy’s clinical course, you administer 3 assessment tools described inTable 3. You explain to Sammy’s parents that these tests will be repeated yearly or when tics worsen. However, you tell his parents that these scores alone will not determine present or future clinical decisions, including treatments. You also recommend that they connect with support groups on the Tourette Syndrome Association (TSA) Web site.
CASE CONTINUED: Changes over time
Sammy’s parents appreciate your explanation and say they will share information from the TSA Web site with Sammy’s principal, teachers, and classmates. The family agrees to return in 6 months or sooner if the tics worsen.
By age 8, Sammy develops multiple tics: facial grimacing, looking upwards, punching movements, whistling, and throat clearing. He is slightly bothered by these tics, and his friends have asked him about them. He tells them he has Tourette syndrome, and that usually ends the questioning. He returns for a follow-up visit because his parents notice a dramatic increase in his tics after Sammy’s father loses his job.
Treatment options
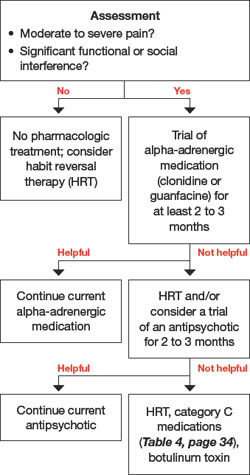
When deciding to treat a child’s tics, the first step is to determine whether to pursue a nonpharmacologic or pharmacologic approach (Algorithm). To tailor an approach most suited for an individual child, discuss with the family their feelings about therapy and medications. This information—along with tic severity—will help determine a treatment plan.
Behavior therapy and medication are management strategies; neither can cure a tic disorder. The most conservative approach to tic treatment is to:
- provide the child and family with basic guidelines for managing tics
- help alleviate environmental stress and other potential triggers.
Algorithm: Recommended treatment of tics in children and adolescents
CASE CONTINUED: A first intervention
You discuss treatment options with Sammy’s family, and they view medication as a last resort. Sammy does not seem to be bothered by his tics, and his parents do not wish to start him on daily medications. Given this situation, habit reversal therapy (HRT) is appropriate for Sammy because he is old enough to participate in HRT to reduce his tics.
HRT is an effective nonpharmacologic approach to help children with tics.4 Its 3 components are:
- awareness training
- competing response training
- social support.5
This simplified version of the original HRT can be completed in eight 1-hour sessions. Good candidates are patients who are cognitively mature enough to understand the therapy’s goals and compliant with frequent clinic visits. They also must practice the strategies at home.
It should not be difficult for psychiatrists to learn HRT—or refer to therapists who are willing to learn it—with the available instructional manual.
CASE CONTINUED: Practicing alternatives
You ask Sammy to imitate his tics. After helping him become more aware of his tics, you encourage him to develop a more socially appropriate movement to engage in whenever he feels the urge to punch. Sammy chooses to clench his fist in his pocket. He also learns to breathe in whenever he has an urge to whistle. you advise Sammy’s parents to reward his efforts to suppress the tics. He practices the strategies daily.
At age 12, Sammy returns to your office. He has begun to have frequent neck-jerking tics, which cause neck pain and daily headaches. He also is slapping his thigh and having frequent vocal tics characterized by loud shrieking. The vocal tics are disruptive in class, even though Sammy sits toward the back of the room. Sammy’s classmates tease him, and he is very frustrated.
Medication approach
The decision to start a medication for tics is complex. Scores from the YGTSS, PUTS, and GTS-QOL scales (Table 3) provide only a partial clinical picture. This decision should be reached after a detailed discussion with the family about benefits and risks of medications and ensuring that everyone’s expectations are reasonable.
A variety of medications are available to treat patients with tics (Table 4). No medication can completely eliminate tics, however, and many have substantial side effects. Before initiating medical treatment, consider 3 questions:
- Is moderate or severe pain involved?
- Is there significant functional interference?
- Is there significant social disruption despite efforts to optimize the social environment for the child?
Sammy’s frequent neck-jerking tics now cause chronic daily headaches, and his shrieking vocal tics are interfering with classroom activities, so we recommended a 3-month trial of guanfacine following the dosing schedule in Table 4.
Table 3
3 scales for assessing tic severity and impact on functioning