Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
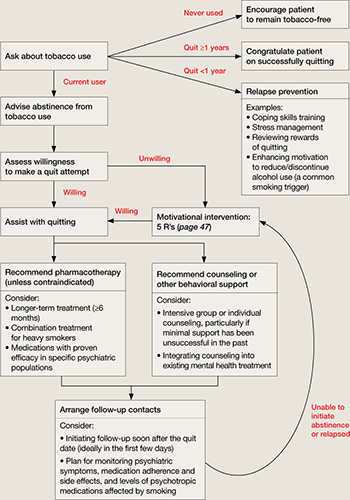
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||