Be sure to include chronic pain or other somatic symptoms in the systems review. Screening tools such as the Visual Analogue Scale can measure pain intensity, while the Cornell Medical Index can uncover somatic symptoms. No all-inclusive tool exists to help detect depression-related somatic symptoms. however.
Should the psychiatrist continue to address Ms. F’s depressive symptoms, or should the focus shift to her somatic symptoms?
Dr. Fishbain’s observations
Patients who do not respond to depression treatment (ie, achieve >50% symptom reduction), or who respond without achieving remission, usually have residual physical symptoms—often fatigue, sleep disturbance, decreased appetite, anxiety, sexual dysfunction, and/or pain.12-14 Severe pain and other somatic symptoms are likely prolonging Ms. F’s depression, despite increased paroxetine dosages.
Paykel et al8 have associated residual depression symptoms with early relapse of depression. In their study, 94% of depressed patients with lingering depressive symptoms had mild to moderate physical symptoms. By contrast, degree of physical symptom improvement has been shown to correlate with likelihood of depression remission.15
Although emotional symptoms improve with antidepressants,16 some evidence17 indicates that physical symptoms associated with depression may be less responsive.
Also, because many psychiatrists have been taught to track emotional symptoms and only some physical symptoms, somatic symptoms of depression often are not targeted for treatment.17 Lack of rating scales to track somatic symptoms compounds this problem.17
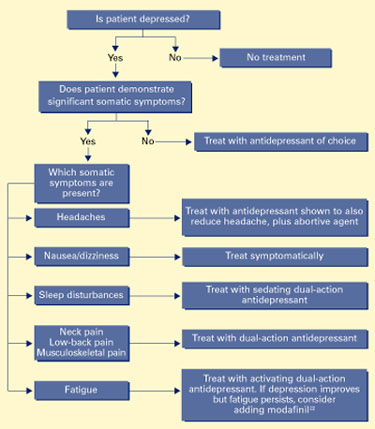
Psychiatrists need to target both the physical and emotional symptoms of depression. When pain prolongs depression, it should be the primary target of antidepressant drug therapy (Algorithm).
To date, several meta-analyses18-20 have demonstrated that antidepressants have a separate analgesic effect on all forms of chronic pain. Evidence21,22 also indicates that the dualaction antidepressants—such as amitriptyline, bupropion, venlafaxine, and (awaiting FDA approval) duloxetine—have a more-consistent analgesic effect than do the serotonin reuptake inhibitors.
The analgesic effects of bupropion, duloxetine, and venlafaxine have not been compared with those of tricyclics or other older antidepressants. If one of the newer dualaction antidepressants does not reduce somatic conditions or produce an adequate response, consider switching to a tricyclic.
Treatment: No pain, some gain
Another psychiatrist who specializes in pain medicine targeted some of Ms. F’s somatic symptoms with antidepressants. Paroxetine and zolpidem were discontinued and the patient was started on:
- venlafaxine, 37.5 mg bid, titrated to 225 mg/d across 2 weeks. Because of its activating properties, venlafaxine was chosen to address Ms. F’s pain and daytime fatigue.
- amitriptyline, 50 mg at bedtime nightly, to promote sleep
- prochlorperazine, 10 mg as needed, and meclizine, 25 mg as needed, to treat her nausea and dizziness, respectively.
Algorithm Suggested drug treatment of depression with somatic symptoms
Ms. F also was advised to take an abortive migraine compound (Midrin, 2 tablets at headache onset and 1 additional tablet every half-hour as needed, maximum 5 tablets per day). Mr. F’s primary care physician also referred her to a physical therapist to treat her neck and low-back pain; workup revealed no surgically treatable problem.
Four weeks later, Ms. F reported that her somatic symptoms significantly improved and that she was sleeping nearly 8 hours per night. Her BDI score was 12, indicating normal mood. She was functioning much more effectively at work and could once again routinely perform her daily activities.
Ms. F continued her medication regimen for 8 months, after which she was lost to follow-up. At her most recent visit, her depression remained in remission. Her pain persisted, though at a lower intensity.
Related resources
- Fishbain DA, Cutler R, Rosomoff HL, Rosomoff RS. Chronic pain-associated depression: antecedent or consequence of chronic pain? A review. Clin J Pain 1997;13:116-37.
Drug brand names
- Amitriptyline • Elavil
- Duloxetine • Cymbalta
- Meclizine • Antivert
- Modafinil • Provigil
- Paroxetine • Paxil
- Prochlorperazine • Compazine
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosure
Dr. Fishbain is a consultant to Eli Lilly and Co. and a speaker for Purdue Pharmaceuticals.