Authors’ Disclosure Statement: Dr. Kovar reports that he receives research support from a company or supplier as a principal investigator from DePuy Synthes, and other financial or material support from a company or supplier from OHK Medical Devices. Dr. Herzenberg reports that he is a consultant for Smith & Nephew, Ellipse Technologies, Orthofix, Orthopediatrics, and Wishbone Medical. He also reports that the following companies supported his institution's non-profit organization, which provides financial assistance to their patients: Stryker; Orthocare Solutions; Medevations; Bay Scribe; Nations Healthcare; and Chesapeake Surgical. The following companies supported Dr. Herzenberg’s institution's annual course for orthopedic surgeons: Smith & Nephew; BrainLab; Orthofix; DePuy Synthes; Stryker; Wright Medical Technology; Zimmer Biomet; and The MHE Coalition. Dr. Jauregui reports no actual or potential conflict of interest in relation to this article.
Dr. Kovar is an Orthopaedic Surgeon, Landesklinikum Baden-Mödling, Austria. Dr. Jauregui is an Orthopedic Surgery Resident, University of Maryland, Department of Orthopedics, Baltimore, Maryland. Dr. Herzenberg is Head of Pediatric Orthopedics, Sinai Hospital, and Director of the International Center for Limb Lengthening, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, Baltimore, Maryland.
Address correspondence to: John E. Herzenberg, MD, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, 2401 W. Belvedere Avenue, Baltimore, MD 21215 (tel, 410-601-9562; fax, 410-601-9575; email, jherzenberg@lifebridgehealth.org).
Am J Orthop. 2018;47(6). Copyright Frontline Medical Communications Inc. 2018. All rights reserved.
Florian M. Kovar, MD Julio J. Jauregui, MD John E. Herzenberg, MD . Accuracy of Distal Femoral Valgus Deformity Correction: Fixator-Assisted Nailing vs Fixator-Assisted Locked Plating. Am J Orthop.
June 12, 2018
References
When using the FAN technique, special attention is paid to reducing the risk of fat embolism. This can be reduced but not totally eradicated with the use of reaming irrigation devices.22-24 In our technique of FAN, the bone is cut and displaced prior to reaming so that the pressure of reaming is vented out through the osteotomy, along with the reaming contents, which theoretically can then act as a “prepositioned bone graft” that may speed healing.
SURGICAL FALP TECHNIQUE
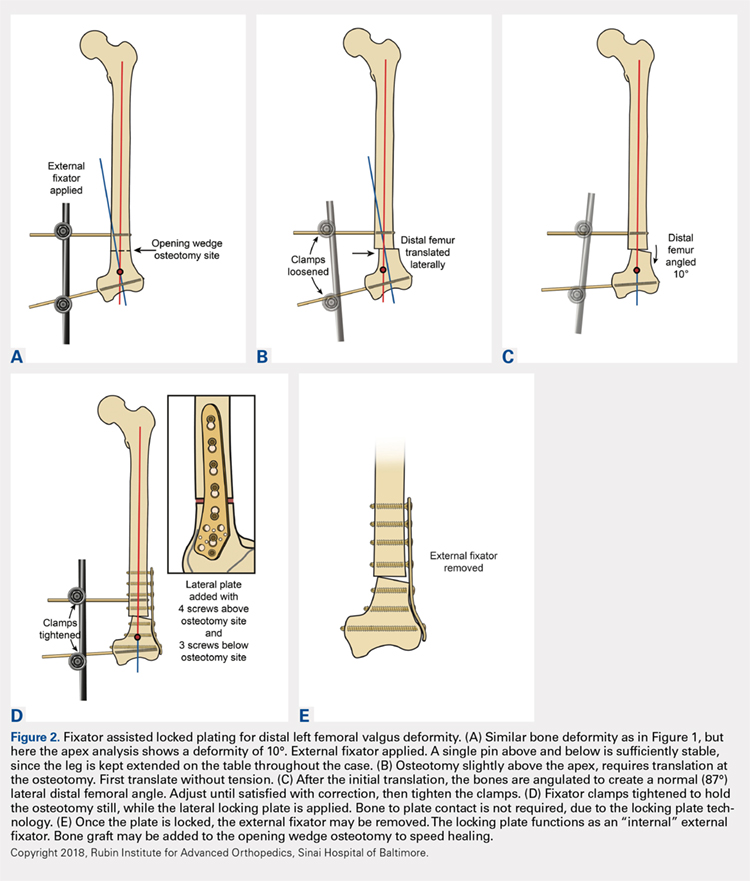
Preoperatively, a decision concerning the planned osteotomy and the correct locking plate size is made. In addition, the outline of the plate is marked on the skin. Under general anesthesia, the patients are prepared and draped. A tourniquet is elevated around the upper thigh. Then, 2 half-pins are medially inserted, 1 proximal and 1 distal to the planned osteotomy site, and are then connected loosely with a monolateral external fixator (Figure 2A). A lateral approach to the distal femur is done, preserving the periosteum, except at the level of the osteotomy. After the osteotomy is performed (through an open lateral incision), both segments are translated (Figure 2B) and then the distal segment is angulated to achieve the desired deformity correction, and the desired position is then stabilized by tightening the external fixator connectors (Figure 2C). Subsequently, a locking plate is inserted in the submuscular-extraperiostal plane. The plate does not require being in full contact (flush) with the bone. At least 3 screws are placed on both sides of the osteotomy through a long lateral incision (Figure 2D). Bone graft may be added to the osteotomy site to encourage healing. Then, the external fixator is removed, and all incisions are closed (Figure 2E).15,19
During each of the procedures, we aimed at having “perfect alignment” with a MAD of 0 mm, in which a Bovie cord is used and passed through the center of the femoral head, knee, and ankle. However, to confirm that the surgery was successful, the actual measurements were performed on standing long-leg films. These films were obtained preoperatively and at latest follow-up. They were performed with the patella aiming forward, the toes straight ahead, feet separated enough for good balance, knees fully extended, and weight equally distributed on the feet. Postoperatively, in both cohorts, partial weight-bearing was encouraged immediately with crutches; physical therapy was instituted daily for knee range of motion. Radiographs were scheduled every 4 weeks to monitor callus formation. Full weight-bearing was allowed when at least 3 cortices were consolidated.1,15,19,20,25,26
All statistical analyses were performed with the aid of the SPSS statistical software package (SPSS). Average values and standard error of the mean were assigned to each variable. A nonparametric Mann-Whitney U test was used, and a 2-tailed P < .05 was considered significant. Correlation of continuous variables was determined by Spearman’s correlation coefficient. Also, multivariate Cox regression analyses after adjustment for age, sex, and deformity correction were used to detect associations within the study population. To evaluate whether our data were normally distributed, Shapiro-Wilk tests were performed.