Authors’ Disclosure Statement: Dr. Kovar reports that he receives research support from a company or supplier as a principal investigator from DePuy Synthes, and other financial or material support from a company or supplier from OHK Medical Devices. Dr. Herzenberg reports that he is a consultant for Smith & Nephew, Ellipse Technologies, Orthofix, Orthopediatrics, and Wishbone Medical. He also reports that the following companies supported his institution's non-profit organization, which provides financial assistance to their patients: Stryker; Orthocare Solutions; Medevations; Bay Scribe; Nations Healthcare; and Chesapeake Surgical. The following companies supported Dr. Herzenberg’s institution's annual course for orthopedic surgeons: Smith & Nephew; BrainLab; Orthofix; DePuy Synthes; Stryker; Wright Medical Technology; Zimmer Biomet; and The MHE Coalition. Dr. Jauregui reports no actual or potential conflict of interest in relation to this article.
Dr. Kovar is an Orthopaedic Surgeon, Landesklinikum Baden-Mödling, Austria. Dr. Jauregui is an Orthopedic Surgery Resident, University of Maryland, Department of Orthopedics, Baltimore, Maryland. Dr. Herzenberg is Head of Pediatric Orthopedics, Sinai Hospital, and Director of the International Center for Limb Lengthening, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, Baltimore, Maryland.
Address correspondence to: John E. Herzenberg, MD, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, 2401 W. Belvedere Avenue, Baltimore, MD 21215 (tel, 410-601-9562; fax, 410-601-9575; email, jherzenberg@lifebridgehealth.org).
Am J Orthop. 2018;47(6). Copyright Frontline Medical Communications Inc. 2018. All rights reserved.
Florian M. Kovar, MD Julio J. Jauregui, MD John E. Herzenberg, MD . Accuracy of Distal Femoral Valgus Deformity Correction: Fixator-Assisted Nailing vs Fixator-Assisted Locked Plating. Am J Orthop.
June 12, 2018
References
RESULTS
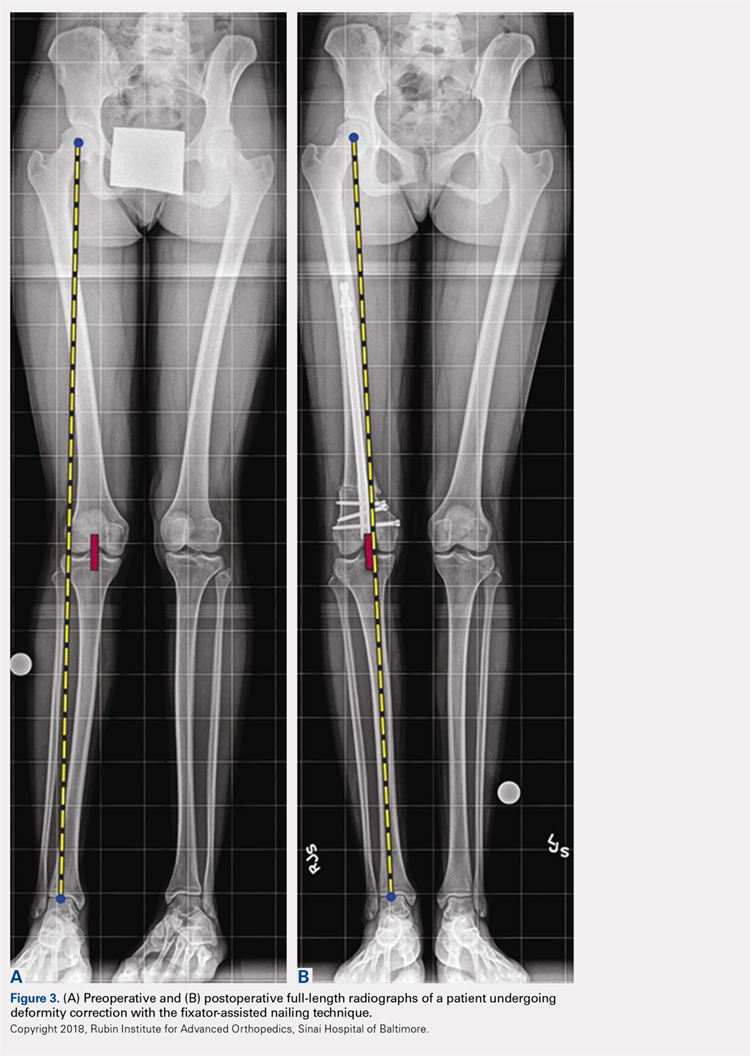
The mLDFA significantly improved in the FAN cohort from a mean of 81° to a mean of 89° (ranges, 67°-86° and 80°-100°; respectively; P = .001) (Figures 3A, 3B).
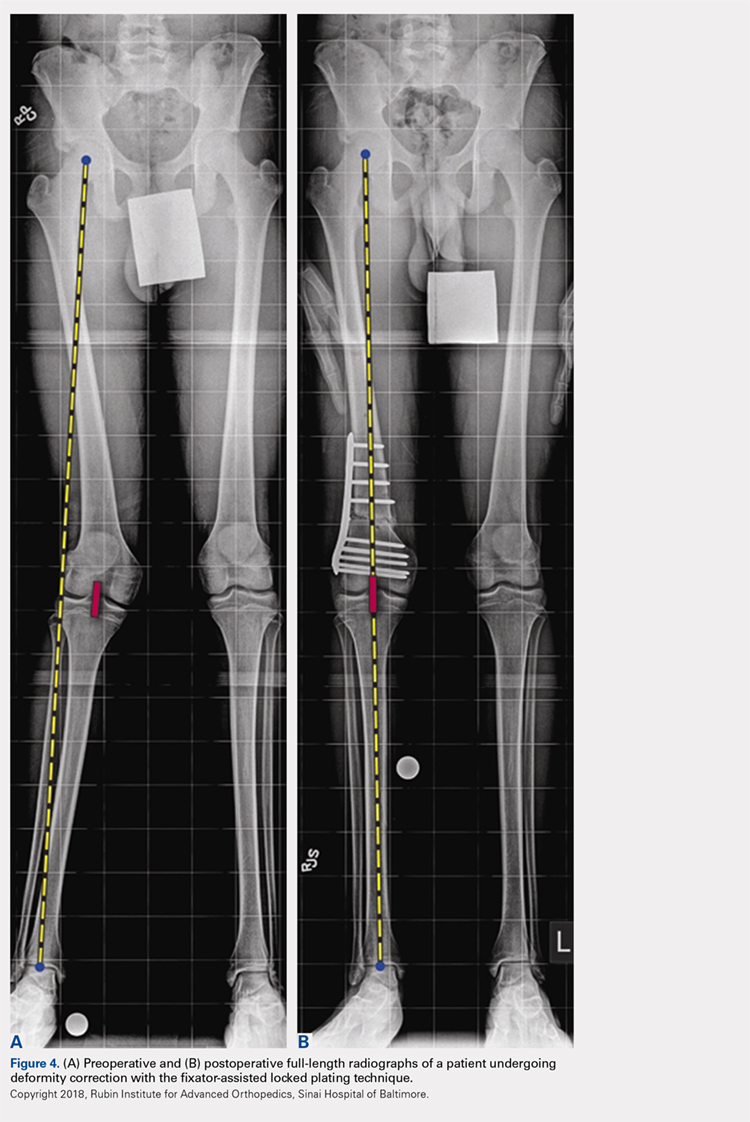
Similarly, the mean mLDFA in the FALP cohort also significantly improved, from 80° preoperatively to 90° postoperatively (range, 71°-87° and 88°-94°, respectively; P < .001) (Figures 4A, 4B).
The mean amounts of correction of mLDFA were 8° (range, 3°-18°) in the FAN group and 10° (range, 7°-17°) in the FALP group (Table 2).
After evaluating the MPTA, in the FAN cohort, we found that the mean pre- and postoperative MPTAs were not modified. These patients had a mean preoperative angle of 88° (range, 62°-100°), which was kept postoperatively to a mean of 88° (range, 78°-96°). In the FALP cohort, a slight change from 90° to 88° was observed (ranges, 82°-97° and 83°-94°, respectively). None of these changes in MPTA were significant (P > .05).
When evaluating correction of the MAD, we observed that the FAN cohort changed from a preoperative MAD of 32 mm (range, 6-64 mm) to a postoperative mean of 10 mm (range, 0-22 mm), and this correction was statistically significant. (P = .001). The FALP cohort changed from a mean of 34 mm (range, 17-62 mm) preoperatively to 4 mm (range, 0-11 mm) postoperatively, and this was also statistically significant (P = .002). The mean MAD correction for the FAN group vs FALP group was 27 mm vs 32 mm, respectively (Table 2).
In patients with valgus femoral deformity, the MAD is usually lateralized; however, in the FAN cohort, we included 3 patients with medial MADs (10 mm, 13 mm, and 40 mm). This is justified in these patients because a complex deformity of the distal femur and the proximal tibia was present. In the extreme case of a 40-mm medial MAD, the presurgery mLDFA was 76°, and the presurgery MPTA was 62°. The amount of deformity correction in this patient was 16°.
During the follow-up period, 2 complications occurred in the FAN group. One patient developed gait disturbance that resolved with physical therapy. Another had an infection at the osteotomy site. This was addressed with intravenous antibiotic therapy, surgical irrigation and débridement, hardware removal, and antegrade insertion of an antibiotic-coated nail. In the FALP group, 1 patient developed a persistent incomplete peroneal nerve palsy attributed to a 17° correction from valgus to varus, despite prophylactic peroneal nerve decompression. Nonetheless, the patient was satisfied with the result, recovered partial nerve function, and returned for correction of the contralateral leg deformity. When comparing the complications between both cohorts, no significant differences were found: 2 of 18 cases (11%) in the FAN group vs 1 of 6 cases (17%) in the FALP group (P = .78).