Author’s Disclosure Statement: The author reports no actual or potential conflict of interest in relation to this article.
Dr. Kiebzak is Orthopedic Research Program Manager, Department of Orthopedics and Sports Medicine, Nemours Children’s Hospital and Specialty Care, Orlando, Florida.
Address correspondence to: Gary M. Kiebzak, PhD, Department of Orthopedics and Sports Medicine, Nemours Children's Hospital and Specialty Care, 13535 Nemours Parkway, Orlando, FL 32827 (tel, 407-264-1368; email, gary.kiebzak@nemours.org).
Am J Orthop. 2018;47(5). Copyright Frontline Medical Communications Inc. 2018. All rights reserved.
Gary M. Kiebzak, PhD . The Potential Value of Dual-Energy X-Ray Absorptiometry in Orthopedics. Am J Orthop.
May 16, 2018
References
CASE SERIES: DISTAL RADIUS FRACTURES
Table 1 summarizes the data comparing radius 33% ROI T-scores and ROI width in patients who fractured the contralateral radius and normal nonfractured controls.10
Table 1. Comparison of Radius Width at the 33% Region of Interest (ROI) and Bone Mineral Density T-Scores in Premenopausal Women With and Without Fractures
33% ROI
T-score
Width of ROI, cm
White women with distal radius fractures
Premenopausal (<49 years), n = 36
-0.2 + 0.9
1.22 + 0.11a
Controls matched for race, age, BMIb
Premenopausal (<49 years), n = 65
-0.1 + 0.8
1.45 + 0.25
aP < 0.0001 compared to matched controls. bControls were women without fractures, who were first randomly matched by race, then age, then body mass index (BMI).
Table 1 was modified with permission from Kiebzak and Sassard.10
For premenopausal women with distal radius fractures, the width of the radius at the radius 33% ROI was significantly smaller than that in controls. However, there was no difference in T-scores between premenopausal women with distal radius fractures and controls. Thus, bone width more accurately identified women with fractures than T-scores based on BMD, and the orthopedist could use bone size in addition to BMD to predict fracture risk in a patient.
PREPARATION FOR SURGERY
For some procedures, there is potential benefit of assessing bone status prior to surgery. That is, determination of low BMD could potentially influence the type of hardware or fixation techniques used in surgery. Various studies have shown that poor bone quality and low BMD can impair purchase with various types of fixation.11-13 Low preoperative BMD has been shown to be related to high implant migration.14 Knowledge of BMD could influence the choice of screw type used or the type of implant metal (titanium vs cobalt chrome). Another example is predicting the risk of spine curvature progression in adolescent idiopathic scoliosis.15-17 It has been reported that low BMD is a risk factor for progression.15 Knowledge of BMD could potentially help with patient management strategies. For example, a patient with low BMD and vitamin D deficiency could be treated (vitamin D supplementation) prior to planning surgery in an effort to improve the low BMD.
PERIOPROSTHETIC BMD
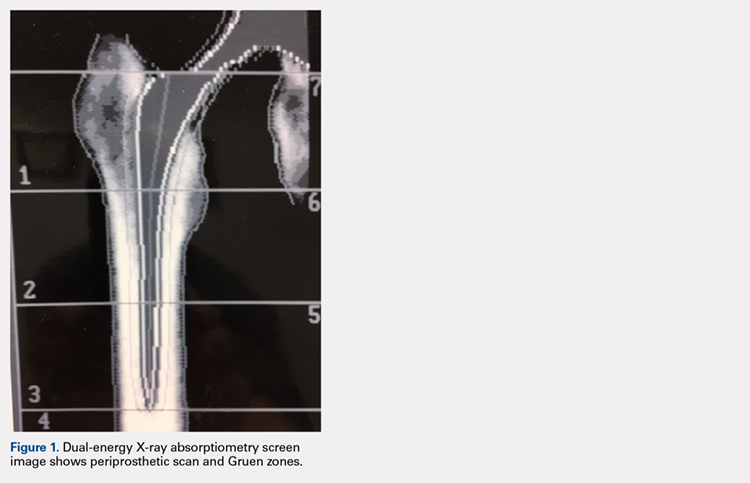
It is possible to monitor changes in BMD around implants using the periprosthetic software application (this usually needs to be purchased separately from standard software that is installed with a system set-up). Dramatic loss of bone due to stress shielding after total hip arthroplasty (THA) can be a risk factor for implant migration or potentially outright failure of fixation or breakthrough. If bone loss occurs and is observed in the early stages, then antiresorptive treatment can be initiated to limit further loss.18,19 (Figure 1) shows the image from a periprosthetic scan.
Standard Gruen zones are the default ROIs.20 It is well established that BMD loss differs from zone to zone, with the greatest loss in zone 7 after THA.