Author’s Disclosure Statement: The author reports no actual or potential conflict of interest in relation to this article.
Dr. Kiebzak is Orthopedic Research Program Manager, Department of Orthopedics and Sports Medicine, Nemours Children’s Hospital and Specialty Care, Orlando, Florida.
Address correspondence to: Gary M. Kiebzak, PhD, Department of Orthopedics and Sports Medicine, Nemours Children's Hospital and Specialty Care, 13535 Nemours Parkway, Orlando, FL 32827 (tel, 407-264-1368; email, gary.kiebzak@nemours.org).
Am J Orthop. 2018;47(5). Copyright Frontline Medical Communications Inc. 2018. All rights reserved.
Gary M. Kiebzak, PhD . The Potential Value of Dual-Energy X-Ray Absorptiometry in Orthopedics. Am J Orthop.
May 16, 2018
References
For older patients being followed after orthopedic care, there is a growing concern about age-related loss of muscle mass, or sarcopenia, which can lead to functional impairment (eg, balance, gait, etc.), and physical disability leading to falling and increased risk of fracture.35-40 Even obese patients can be sarcopenic (a concept known as sarcopenic obesity), and their large body mass can mask the relative deficiency of lean mass.40 DXA total body scans can be used to monitor patients at risk for sarcopenia.
Finally, DXA total body composition scans are underused in the pediatric population. Given the low radiation burden, DXA can be used safely in children of all ages. In addition to the same uses as in adults for presurgical assessment, monitoring bone and soft-tissue changes after treatment and rehabilitation, scans can be used to monitor growth and development.41
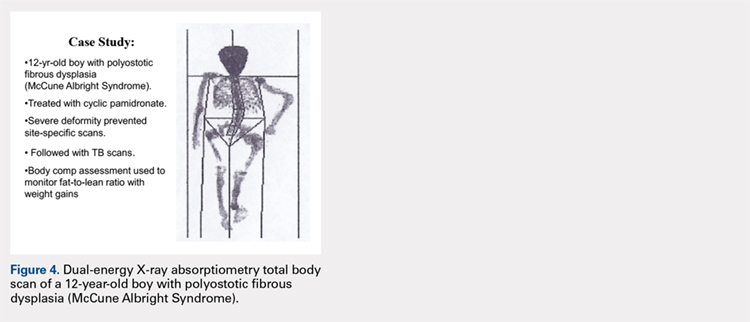
CASE STUDY: MONITORING DEVELOPMENT AND TREATMENT
A 12-year-old boy with polyostotic fibrous dysplasia (McCune Albright Syndrome) was started on treatment with cyclic pamidronate to mitigate bone pain and reduce fracture risk. Use of DXA was planned to provide evidence of treatment efficacy by documenting increasing BMD. However, the severe skeletal deformity prevented standard site-specific DXA scans, and consequently, total body scans were effectively used to acquire the BMD data needed to monitor treatment (Figure 4).
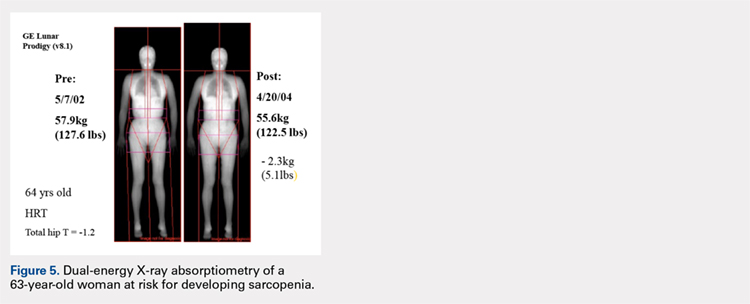
CASE STUDY: AGE-RELATED SARCOPENIA
Figure 5 shows images of a 64-year-old woman who was followed after a distal radius fracture. A total body scan and body composition assessment was performed in 2002. At follow-up in 2004, total body weight seemed stable with only a seemingly benign 5.1-lb loss of weight, and the patient’s overall physical appearance was unchanged (Table 2).
Table 2. Age-Related Changes Potentially Leading to Sarcopenia
Baseline, 2002
Follow-up, 2004
Change, %
Body weight, kg
57.9 (127.6 lb)
55.6 (122.5 lb)
4
BMI
20.6
19.8
Total body fat, g
13,619
13,390
−1.7
Total body percent fat
23.5
24.1
Total body lean, g
42,038
39,949
−5.0
Dual-energy X-ray absorptiometry scans were performed using a GE Lunar Prodigy system.
However, body composition assessment revealed a disproportionate loss of lean mass, with a resultant total percent body fat increase. This imbalance between the change in fat and lean mass could lead to clinical sarcopenia unless appropriate dietary and exercise measures are taken. Such subtle developing imbalances in body composition could only be quantitated using DXA total body scans.