WHAT ARE THE MEDICAL OPTIONS?
Initial management of ABS in children is contingent on the symptom profile at presentation (persistent, worsening, or severe) and consideration of causative pathogens. While the consensus among experts is that children presenting with severe or worsening symptoms be treated initially with antibiotics,3,4 children who present with mild symptoms consistent with persistent illness may initially be treated with antibiotics or observed for an additional three days. This decision should be made thoughtfully and in collaboration with the patient’s parents or guardians. Any child with ABS who presents with persistent symptoms of illness and is managed initially by observation alone should be reassessed or treated with an antibiotic if symptoms worsen, if new symptoms appear, or if the child fails to improve within 72 hours.
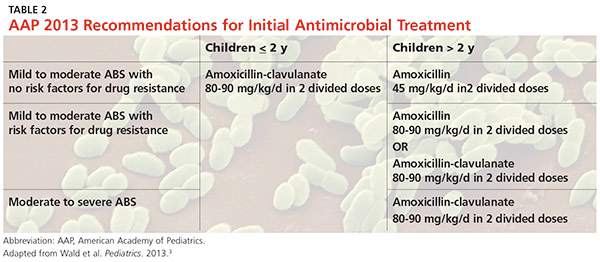
Amoxicillin with or without clavulanate is the antibiotic of choice when ABS has been diagnosed and antibiotic treatment is indicated.1,3 AAP recommendations for antimicrobial treatment of ABS in children are stratified on the basis of age, severity of illness, day care attendance, and history of treatment with amoxicillin in the previous 30 days (see Table 2). Clinicians should rely on their knowledge of drug resistance in their community and judgment regarding severity of illness when choosing between amoxicillin and amoxicillin/clavulanate as initial treatment for ABS.3
Recommendations for duration of antimicrobial treatment for ABS vary considerably. A reasonable suggestion is to continue to treat patients until they are symptom-free for seven days. For many patients, this will mean a 10-day treatment course, with flexibility to increase the duration as needed.3
Children with ABS should be reassessed if there are worsening signs or symptoms or lack of clinical improvement within 72 hours of initial management. Clinicians should evaluate whether the patient has been appropriately diagnosed and assessed for complications of ABS. If the diagnosis is confirmed and ABS complications are not suspected, the clinician may change antibiotics or initiate antibiotic therapy if the child was previously managed by observation only.3,4
A child who is vomiting or unable to tolerate PO medications may benefit from a single 50-gm/kg dose of ceftriaxone IV or IM with follow-up in 24 hours.3 Oral antibiotics may be started at the follow-up visit if the patient demonstrates clinical improvement.
When considering a change in antibiotic, the clinician should consider the possibility of drug resistance. If the child was initially treated with amoxicillin, high-dose amoxicillin/clavulanate may be prescribed. If high-dose amoxicillin/clavulanate was initially prescribed and the patient has not improved or is experiencing worsening symptoms, clindamycin with cefixime, linezolid with cefixime, or levofloxacin may be considered.3,4
Penicillin allergy
Patients with a history of a non–type 1 hypersensitivity reaction to amoxicillin may be treated with cefdinir, cefuroxime, cefpodoxime, or combination therapy with clindamycin plus a third-generation oral cephalosporin. Allergist referral for penicillin or cephalosporin skin testing may be considered before initiation of therapy.3,4,13
Adjuvant therapy
Decongestants, antihistamines, and nasal irrigation are frequently recommended in the management of ABS in children; however, the authors of a 2012 Cochrane review found no properly designed studies to evaluate the effectiveness of these treatments.13 Furthermore, there is insufficient evidence to clearly recommend the use of intranasal steroids as an adjuvant therapy in the treatment of ABS in children (although several randomized controlled studies demonstrate their effectiveness in adolescents and adults).3
Continue for the conclusion >>