The interview should be concise, with the patient’s account of the assault recorded in some way so that he or she can later be quoted as closely as possible. The clinician should avoid using medical or legal terms or abbreviations, or altering the patient’s own words.
Before the physical examination is begun, the patient’s clothing must be collected and each piece packaged in a separate paper bag. Women’s underpants are the garment most likely to contain “transfer from the perpetrator.”10
Julie had changed her clothes before coming to the ED but was wearing the same underpants she had on at the time of the assault. This garment was collected in a paper bag.
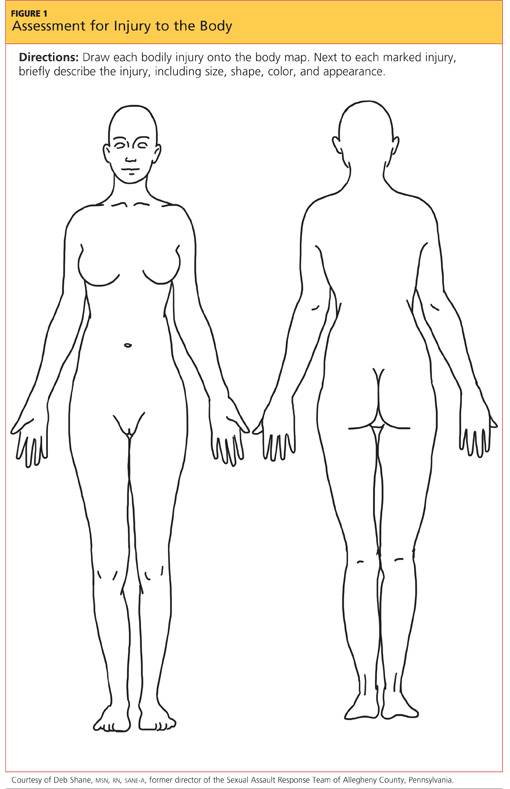
The physical exam is conducted in a head-to-toe manner. Each marking found on the victim must be charted on a diagram of the body or the genitalia (see Figure 1). Injuries should be described using the mnemonic TEARS: tissue integrity, ecchymoses, abrasions, redness, and swelling.11 The most common descriptors include abrasions that are tangential or patterned, fingernail markings, contusions, and lacerations.
When the clinician examines the patient’s genitalia and anal area, it is important to report a thorough description of any injuries. The most common area of injury in the female sexual assault victim is a small tear to the posterior fourchette. Visualization can be enhanced by use of toluidine blue dye—but this must be applied before use of a speculum,12 and not until after any photographs of the outer genitalia have been taken.
Photographs should be taken of all injuries, then presented to the police. It is suggested that each injury be photographed from a medium distance, and up close with a ruler or other scale.7
Julie stated that she had been a virgin prior to the assault. She was placed in the lithotomy position, and a careful internal inspection was performed. Gentle retraction of the labia with a good light source allowed adequate visualization. Photographs were taken of an acute laceration of the hymen at the 5:00 position.
PHYSICAL EVIDENCE
Next, evidence is collected from the patient’s body. Fingernails are clipped and saved for possible DNA from the suspect, especially if the victim reports having tried to fight back. The fingernail trimmings from each hand should be packaged separately, with labels.7
Debris is combed from the head hair and pubic hair. This can be significant for confirming details from the victim’s story, such as being attacked and thrown into the mud. Next, the patient’s head hair is collected. When plucking the hair, the examiner must ensure that the root is intact, since the patient’s DNA is contained therein. This can be important for distinguishing the patient’s hair from that of the suspect. Hairs should be chosen from a few different areas of the patient’s head.7
Oral, genital, and anal swabs are collected. For collection of evidence from a female patient, a speculum exam is required.12 The vagina is swabbed with at least four different cotton swabs: one for the cervix, and the other three to collect visualized secretions.10 For each area, a clean, sterile swab should be moistened with distilled water and used to swab lightly, rotating downward. A dry sterile swab is then used to re-swab the area lightly and lift the DNA. Collected swabs should be allowed to dry completely before the packaging is sealed to minimize the risk for contamination by bacterial growth.
Use of a Wood’s lamp can help the examiner detect semen and saliva on the patient’s body.10 However, a recent examination of alternate light sources with appropriate wavelengths has demonstrated improved detection of trace DNA evidence.13
Once the steps in evidence collection have been completed, the patient can be permitted to urinate, shower, brush his or her teeth, and make any necessary phone calls.
Storing and Protecting the Evidence
It is imperative for the NP or PA who completes the kit to maintain the chain of custody—that is, never leaving the evidence unattended until the police collect it. This will eliminate the possibility of tampering or any other reason for the legal system to designate the evidence as inadmissible. If it is not feasible for the responsible clinician to guard the evidence, it must be placed under lock and key, with limited availability to others.10
Evidence that cannot be thoroughly dried during the examination (eg, tampon, condom, tissues) should be collected in a sterile specimen cup and sent to the crime lab immediately.7 Otherwise, if such a sample is packaged and left to sit, the risk increases for any DNA to become contaminated by bacterial growth.