

Commentary

Physician Advocacy for Zoster Vaccination
Herpes zoster (HZ) infection occurs when the varicella-zoster virus (VZV) is reactivated due to waning cellular immunity associated with age or...
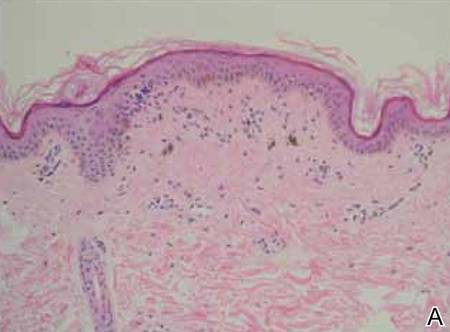
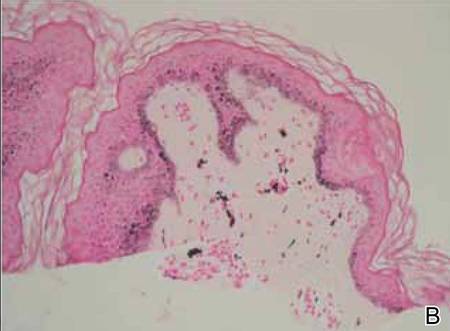
Progressive cribriform and zosteriform hyperpigmentation (PCZH) was first described in 1978. The diagnostic criteria included the following: (1) uniformly tan cribriform macular pigmentation in a zosteriform distribution; (2) a histologic pattern that consisted of a mild increase in melanin pigment in the basal cell layer and complete absence of nevus cells; (3) no history of rash, injury, or inflammation to suggest postinflammatory hyperpigmentation; (4) onset occurring well after birth with gradual extension; and (5) lack of other associated cutaneous or internal abnormalities. Many pigmentary disorders occurring along the Blaschko lines are included in the differential diagnosis of PCZH.
Herpes zoster (HZ) infection occurs when the varicella-zoster virus (VZV) is reactivated due to waning cellular immunity associated with age or...
We present a case of lichen striatus (LS) in a 36-year-old woman with skin lesions on the right side of the chest distributed along Blaschko lines...