Case Report
A 57-year-old black woman with a history of dialysis-dependent end-stage renal disease, diabetes mellitus (DM), hypertension, diastolic congestive heart failure, and chronic bronchitis was admitted to Howard University Hospital (Washington, DC) for acute chest pain and shortness of breath. During her hospital stay the dermatology team was consulted for evaluation of two 1.6-cm teardrop-shaped, yellow-white-chalky plaques noted in the center of an atrophic, hyperpigmented, shiny, contracted split-thickness skin graft (STSG) on the right posterior forearm (Figure 1). Twenty years prior, the patient received STSGs on the right and left forearm secondary to caustic burns. Two months before the current admission she noticed 2 adjacent teardrop-shaped white plaques within the center of the STSG on the right forearm. At a 3-month follow-up, she had developed more lesions within both graft sites of the bilateral forearm. There was no notable pruritus associated with the lesions.

Figure 1. Acquired perforating dermatosis of the right posterior forearm at the site of a split-thickness skin graft showing discrete, well-demarcated, teardrop-shaped, yellow-white-chalky plaques.
A 4-mm punch biopsy showed an orthokeratotic plug with basophilic inflammatory debris adjacent to acanthotic epidermis, necrotic basophilic debris at the superficial dermis with epidermal canals extending from the base of the lesion superiorly, and transepidermal elimination of elastic fibers (Figure 2A). A Verhoeff-van Gieson stain revealed the necrotic basophilic debris located in the superficial dermis admixed with a cluster of black wavy elastic fibers establishing the identity of the perforating substance (Figure 2B). Masson trichrome stain revealed loss of collagen structure within the aggregate of elastic fibers adjacent to the epidermis and no collagen within epidermal canals (Figure 2C). These histopathologic findings together with the clinical presentation were consistent with a diagnosis of acquired perforating dermatosis (APD).
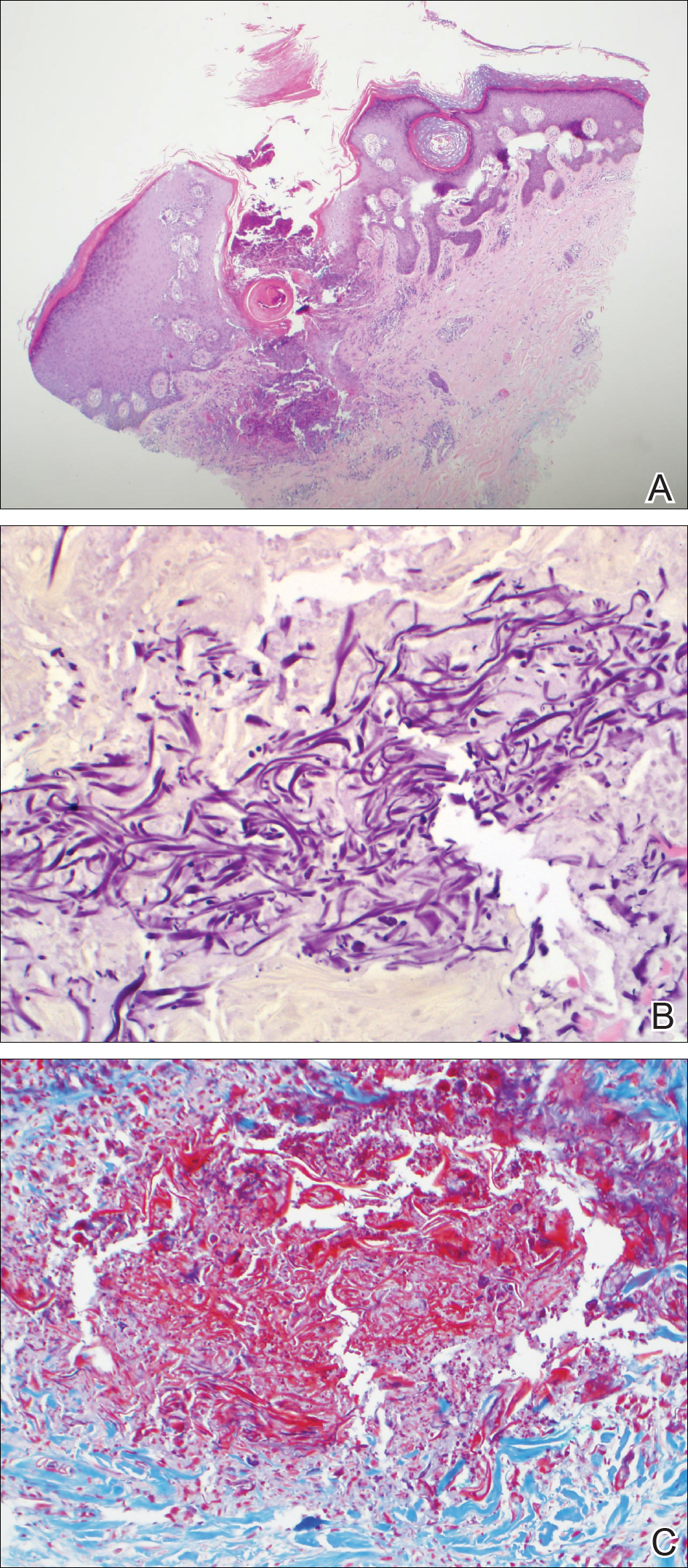
Figure 2. Histopathology of acquired perforating dermatosis at the site of a split-thickness skin graft revealed a cuplike depression of an orthokeratotic plug with basophilic inflammatory debris adjacent to acanthotic epidermis, basophilic debris at the superficial dermis with epidermal canals extending from the base of the epidermis, and transepidermal elimination of elastic fibers (A)(H&E, original magnification ×4). Verhoeff-van Gieson stain demonstrated black wavy elastic fibers in the superficial dermis at the base of the epidermis (B)(original magnification ×40). Masson trichrome stain showed loss of collagen structure within the aggregate of elastic fibers adjacent to the epidermis (C)(original magnification ×20).